On this page
Pyomyositis is an infection of the muscle, almost always due to Staphylococcus aureus. It most commonly affects the muscles of the limbs and torso. Infections may occur simultaneously in multiple sites.
Risk factors include immunosuppression, concurrent S. aureus infection, malnutrition, trauma and injection drug use. Risk of mortality is significant if treatment is delayed.
Clinical features
- Signs and symptoms:
- local: exquisite muscle tenderness, oedema giving muscles "woody" texture on palpation.
- systemic: regional adenopathy and fever.
- pyomyositis of the psoas muscle: patient keeps hip flexed and experiences pain on hip extension. If the abscess is on the right side, the clinical signs are the same as for appendicitis with pain in the right iliac fossa.
- Complications: septic emboli, endocarditis and septic arthritis, septic shock (see Shock, Chapter 1).
Paraclinical investigations
- POCUSaCitation a.POCUS should only be performed and interpreted by trained clinicians.: assists in characterisation of abscess; can rule out deep venous thrombosis.
- Radiography: may demonstrate a foreign body, signs of osteomyelitis or osteosarcoma.
Treatment
- Immobilise the limb.
- Systematic antibiotic therapy (see Erysipelas and cellulitis, Chapter 4).
- Adapt analgesics to the pain level (see Pain, Chapter 1).
- Apply compresses soaked in 70% alcohol 2 times daily (max. 3 times daily to prevent burns to the skin) until incision and drainage.
- Treatment is surgical incision and drainage, under aseptic conditions (sterile consumables and instruments, antiseptic skin preparation) following the rules for incision and drainage of abscesses (see Cutaneous abscess, Chapter 10). Muscle abscesses are often deeper than other abscesses. As a result, aspiration with a large bore needle may be necessary to locate the abscess. Needle aspiration is insufficient treatment even if pus is evacuated and should be followed by surgical incision and drainage.
- In case of pyomyositis of the psoas muscle, start antibiotics and refer to a surgeon.
Equipment and anaesthesia
As for Cutaneous abscess, Chapter 10.
Technique
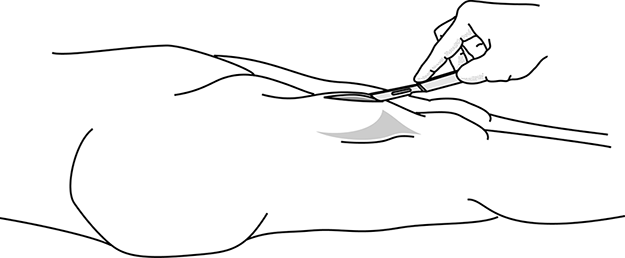
- Generous incision along the axis of the limb, over the site of the abscess and avoiding underlying neurovascular stuctures; incise the skin, subcutaneous tissues and muscular fascia with a scalpel (Figure 9a).
- Dissect the muscle fibres with non-toothed forceps (Kelly type) or round tipped scissors. Insert the instrument or a finger into the muscle until the purulent cavity is reached. If an instrument is used, during insertion, keep the instrument closed and perpendicular to the muscle fibres. Withdraw gently with the scissors or forceps slightly open, keeping instrument perpendicular to the fibres (Figure 9b). If abscess is found to be very deep, it may be necessary to refer to a surgeon.
- Use a forefinger to explore the cavity, break down any loculi and evacuate the pus (Figure 9c).
- Wash abundantly with 0.9% sodium chloride.
- Insert a large drain.
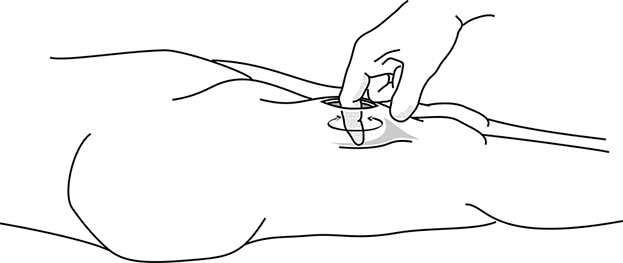
- Fix the drain to the edge of the wound using a single suture. Remove the drain on about the 5th day (Figure 9d).
Figures 9: Surgical incision-drainage of a pyomyositis
|
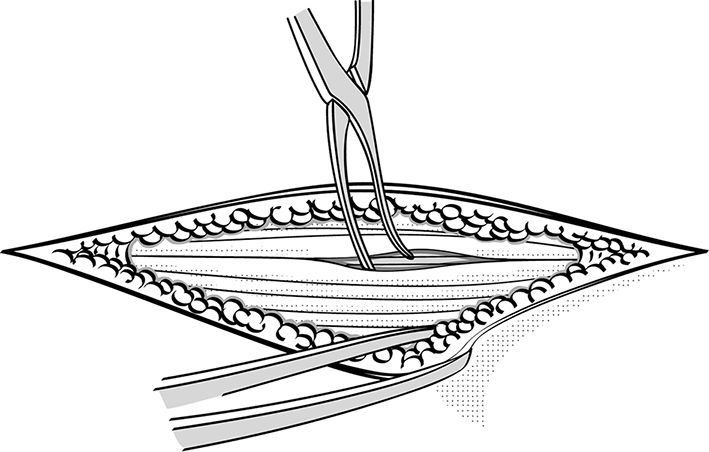 Figure 9b Dissection of the muscle using Kelly forceps, insert closed then withdraw with the instrument slightly open |
|
 Figure 9d Drain fixed to the skin |
Notes
- (a)POCUS should only be performed and interpreted by trained clinicians.