For more information, refer to these documents:
http://whqlibdoc.who.int/publications/2009/9789241597555_eng.pdf
|
The measles vaccine is a live, attenuated virus vaccine.
2.1.1 Composition
Most of the vaccines currently in use are derived from the Edmonston strain of the measles virus: Schwarz, Edmonston-Zagreb, AIK-C and Moraten. Vaccines derived from other strains are also available: CAM-70, TD-97, Leningrad-16 and Shanghai-191.
There is no significant difference (in terms of efficacy and adverse effects) between these vaccines, and all strains may be used interchangeably.
The vaccines may contain stabilisers (sorbitol or hydrolyzed gelatine) and a small amount of neomycin, but no thiomersal.
2.1.2 Dose and route of administration
Children under 2 years: 0.5 ml per dose, IM route, anterolateral thigh
Children 2 years and over, adolescents and adults: 0.5 ml per dose, SC route, lateral upper arm
2.1.3 Age and vaccine response
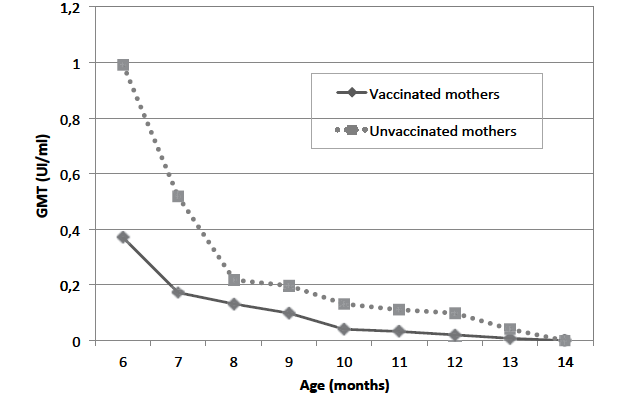
The persistence of maternal antibodies affects the vaccine response. Depending on the titre of passively acquired maternal antibodies, infants are in theory protected until age 6 to 9 months. Children born to mothers who were vaccinated in childhood are not protected for as long as those whose mothers are protected naturally by the disease (Figure 2.1).
Figure 2.1: Placental transfer and change in antibody titre with age according to mother’s vaccination status [1]Citation 1.Pinquier D., et al. Distribution of serum measles-neutralizing antibodies according to age in women of childbearing age in France in 2005-2006: impact of routine immunization. Pediatr Infect Dis J 26(8):749-50 (2007).
The optimal age for vaccination (first and second doses) varies depending on the local epidemiological situation. It is a trade-off between the child’s risk of contracting the illness during the first few months of life and the need to get a high seroconversion rate.
When the first dose of vaccine is administered to children ages 9 to 12 months, the seroconversion rate is about 85%. This increases to 90-95% when children are vaccinated at 12 months. Several studies have tended to show that seroconversion is even higher if the vaccine is administered at 15 months, but does not increase further if the vaccine is administered beyond age 15 months.
Seroconversion appears 10 to 14 days after vaccination, with a peak between the 21st and 28th days.
The protection conferred by primary vaccination lasts several dozen years. Without a second dose the antibody level declines over time, but immune memory persists. When a vaccinated person is exposed to the virus, the immune response is rapidly reactivated.
In order to reduce the number of susceptibles, all children must receive a second dose of vaccine. It is administered after age 1 year, and in most cases allows seroconversion in children who failed to respond to primary vaccination or catch-up for children who never received it.
2.1.4 Contraindications
- History of anaphylactic reaction to any of the vaccine’s components (neomycin orgelatine) or to a previous measles vaccine injection.
- Severe immune deficiency (known or clinically suspected):
- congenital or acquired;
- HIV infection: children who are symptomatic and/or whose CD4 ≤ 25%;
- leukaemia, advanced lymphoma, or serious neoplastic disease;
- immunosuppressant drugs (high-dose corticosteroids, antineoplastic chemotherapy, etc.).
- Ongoing severe acute infection. A minor infection is not a contraindication.
2.1.5 Special situations
Malnutrition
Most studies have shown that the immune response to vaccination is the same in nonmalnourished and malnourished children. Malnutrition increases the risk of contracting the disease and developing severe complications [2]Citation 2.Bhaskaram P. Measles and malnutrition. Indian J Med Res. 1995 Nov;102:195-9. . Malnourished children are routinely vaccinated in feeding programmes.
Pregnancy
Measles often causes severe complications both for the mother and the foetus (spontaneous abortion) or newborn (congenital measles).
In principle, live vaccines should not be administered to pregnant women. However, during an epidemic in which there are adult cases, the risk/benefit of vaccination should be discussed.
HIV infection
[3]Citation 3.Scott P, Moss WJ, Gilani Z, Low N. Measles vaccination in HIV-infected children: systematic review and meta-analysis of safety and immunogenicity. J Infect Dis. 2011 Jul;204 Suppl 1:S164-78. doi: 10.1093/infdis/jir071., [4]Citation 4.Centers for Disease Control and Prevention. General Recommendations on Immunization. Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity and Mortality Weekly Report. December 1, 2006 / Vol. 55 / No. RR-15.
http://www.cdc.gov/mmwr/pdf/rr/rr5515.pdf
All HIV-infected children without severe immune deficiency should be vaccinated as soon as possible.
In immunodepressed children, the first dose of vaccine is administered after immune function is restored (generally after 6 to 12 months of antiretroviral therapy):
- CD4 > 25% in children under 5 years;
- CD4 > 200 in children 5 years and older.
The second dose is administered at least 4 weeks after the first.
Immunoglobulins and other blood products
If a child has received immunoglobulins or blood products 3 to 6 months before vaccination or within 2 weeks after vaccination, administer an additional dose of vaccine 3 to 6 months later.
Prolonged corticosteroid therapy
Patients receiving ≥ 2 mg/kg daily of prednisolone are vaccinated:
- as soon as treatment is stopped if the duration of treatment is < 14 days;
- one month after treatment is stopped if the duration of treatment is ≥ 14 days.
2.1.6 Adverse effects
Adverse effects are generally minor and transient.
- In the first 24 hours, mild pain and tenderness at the injection site.
- 7 to 12 days after vaccination:
- fever > 39 °C lasting 1 to 2 days in 5 to 15% of cases; the fever can sometimes cause seizures (1/3000);
- transient skin rash in 2% of cases, sometimes with catarrhal symptoms;
- rarely: thrombocytopenic purpura (1/30,000 to 1/100,000);
- very rarely: encephalitis (1/1 million).
- Anaphylactic reactions to one of the components of the vaccine: rare (1/20,000 to 1/1 million).
With the exception of anaphylactic reactions, there is a smaller risk of adverse reactions from the second dose.
2.1.7 Combination vaccines and co-administration of multiple vaccines
Combination vaccines
Vaccines come in either monovalent or combined form, that is, associated with other vaccines in the same syringe. The available combination vaccines are:
- MR: measles and rubella;
- MMR: measles, mumps and rubella;
- MMRV: measles, mumps, rubella and varicella.
Co-administration of multiple vaccines
Provided different syringes and different injection sites are used, measles vaccine can be administered at the same time as most other vaccines: DTP, hepatitis B, Haemophilus influenzae, oral or inactivated polio, yellow fever, varicella, pneumococcal, meningococcal (polysaccharide AC, conjugate A).
Giving it at the same time as Japanese encephalitis vaccine also appears possible, but further studies are needed to validate this.
To avoid the risk of one immune response interfering with another, different live vaccines should be administered at least four weeks apart.
2.1.8 Vaccine storage
Lyophilised vaccine
To be kept refrigerated between +2 °C and +8 °C. Long term storage in temperatures between –70 °C and –20 °C is possible but is no longer recommended.
Diluent
To be stored at room temperature. However, at least 12 hours before reconstitution, it should be placed in the refrigerator to avoid thermal shock to the lyophilised vaccine (a temperature difference may reduce vaccine efficacy). Do not freeze.
Reconstituted vaccine
The reconstituted vaccine is sensitive to heat and light. It must be kept refrigerated between +2 °C and +8 °C, protected from light, and used within 6 hours after reconstitution.
- 1.Pinquier D., et al. Distribution of serum measles-neutralizing antibodies according to age in women of childbearing age in France in 2005-2006: impact of routine immunization. Pediatr Infect Dis J 26(8):749-50 (2007).
- 2.Bhaskaram P. Measles and malnutrition. Indian J Med Res. 1995 Nov;102:195-9.
- 3.Scott P, Moss WJ, Gilani Z, Low N. Measles vaccination in HIV-infected children: systematic review and meta-analysis of safety and immunogenicity. J Infect Dis. 2011 Jul;204 Suppl 1:S164-78. doi: 10.1093/infdis/jir071.
- 4.Centers for Disease Control and Prevention. General Recommendations on Immunization. Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity and Mortality Weekly Report. December 1, 2006 / Vol. 55 / No. RR-15.
http://www.cdc.gov/mmwr/pdf/rr/rr5515.pdf