A cutaneous abscess is a collection of pus within the dermis or subcutaneous tissue.
It is most commonly due to Staphylococcus aureus.
Clinical features
- Painful, red, shiny nodule with or without fluctuance; suppuration or surrounding cellulitis (see Erysipelas and cellulitis, Chapter 4).
- Regional adenopathy and fever may be present.
- Complications: osteomyelitis, septic arthritis, septic shock (see Shock, Chapter 1).
Paraclinical investigations
Radiography in case of suspected osteomyelitis or septic arthritis.
Treatment
- Treatment is surgical incision and drainage, under aseptic conditions (i.e. sterile consumables and instruments, antiseptic skin preparation).
- Refer to a surgeon any cutaneous abscess:
- located in anterior and lateral neck, central triangle of the face, hand, perirectal region, breast, or
- adjacent to major blood vessels (e.g. femoral artery), or
- involving joint and bone.
- Antibiotic therapy only if signs of systemic infection, extensive surrounding cellulitis or for individuals with risk factors e.g. immunosuppression or diabetes (for antibiotic therapy, see Erysipelas and cellulitis, Chapter 4).
Equipment
- Sterile scalpel
- Sterile curved, non-toothed artery forceps (Kelly type)
- Sterile disposable gloves and compresses
- Antiseptic solution and 0.9% sodium chloride
- 5 or 10 ml syringe
Anaesthesia
- For small (approximately < 5 cm), well delineated abscess in adults: use local anaesthesia with 1% lidocaine without epinephrine (10 mg/ml): 15 to 20 ml.
- For larger (approximately > 5 cm), deep or poorly delineated abscess in adults or for abscess in children: consider procedural sedation or general anaesthesia (ketamine IM: 10 mg/kg).
For analgesia, see Pain, Chapter 1.
Technique
Incision
(Figure 8a)
- Hold the scalpel between the thumb and middle finger of the dominant hand, the index finger presses on the handle. Hold the abscess between the thumb and index finger of the other hand. The scalpel blade should be perpendicular to the skin.
- The incision is made in a single stroke along the long axis of the abscess. The incision must be long enough for a finger to be inserted.
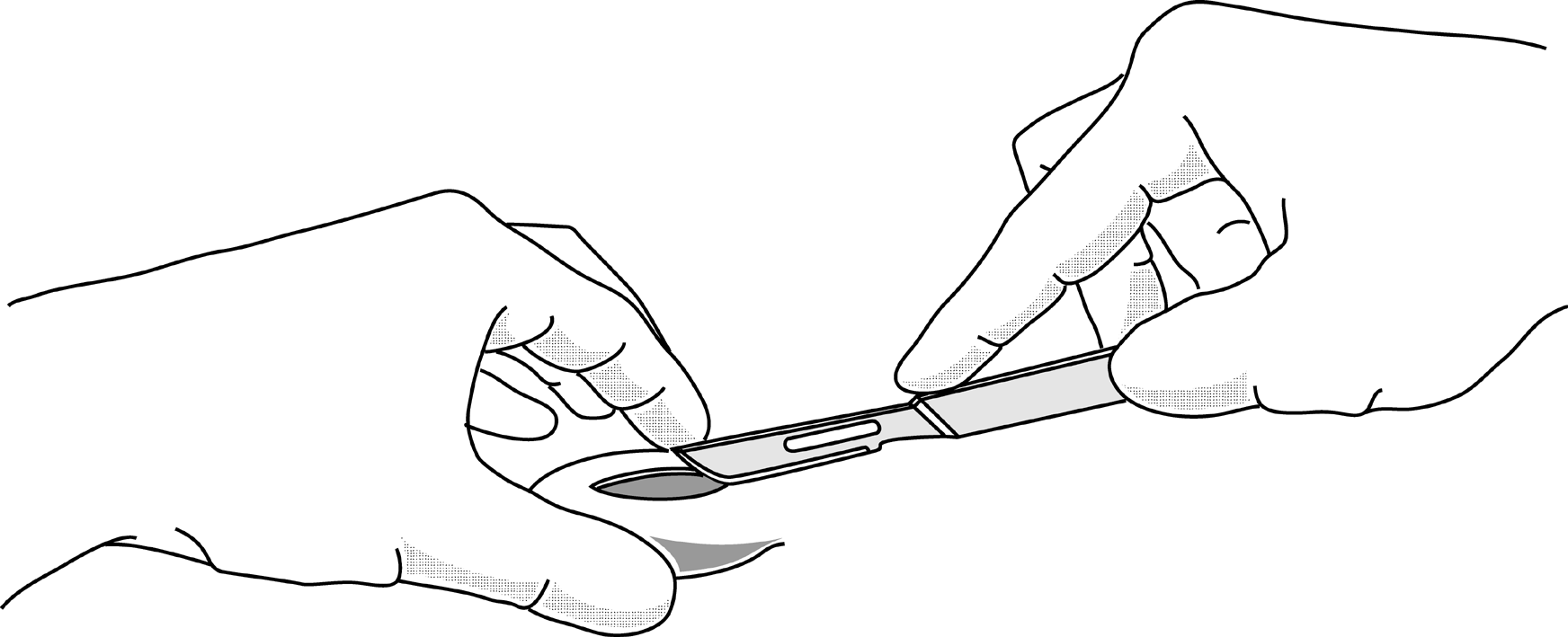
Figure 8a |
Digital exploration
(Figure 8b)
- Explore the cavity with the index finger, breaking down all loculi (a single cavity should remain), evacuate the pus (and foreign body, if present) and explore to the edges of the cavity.
- The exploration also allows an assessment of the extent of the abscess, the depth, and location with respect to underlying structures (arterial pulsation) or any possible contact with underlying bone. In this last case, seek surgical advice.
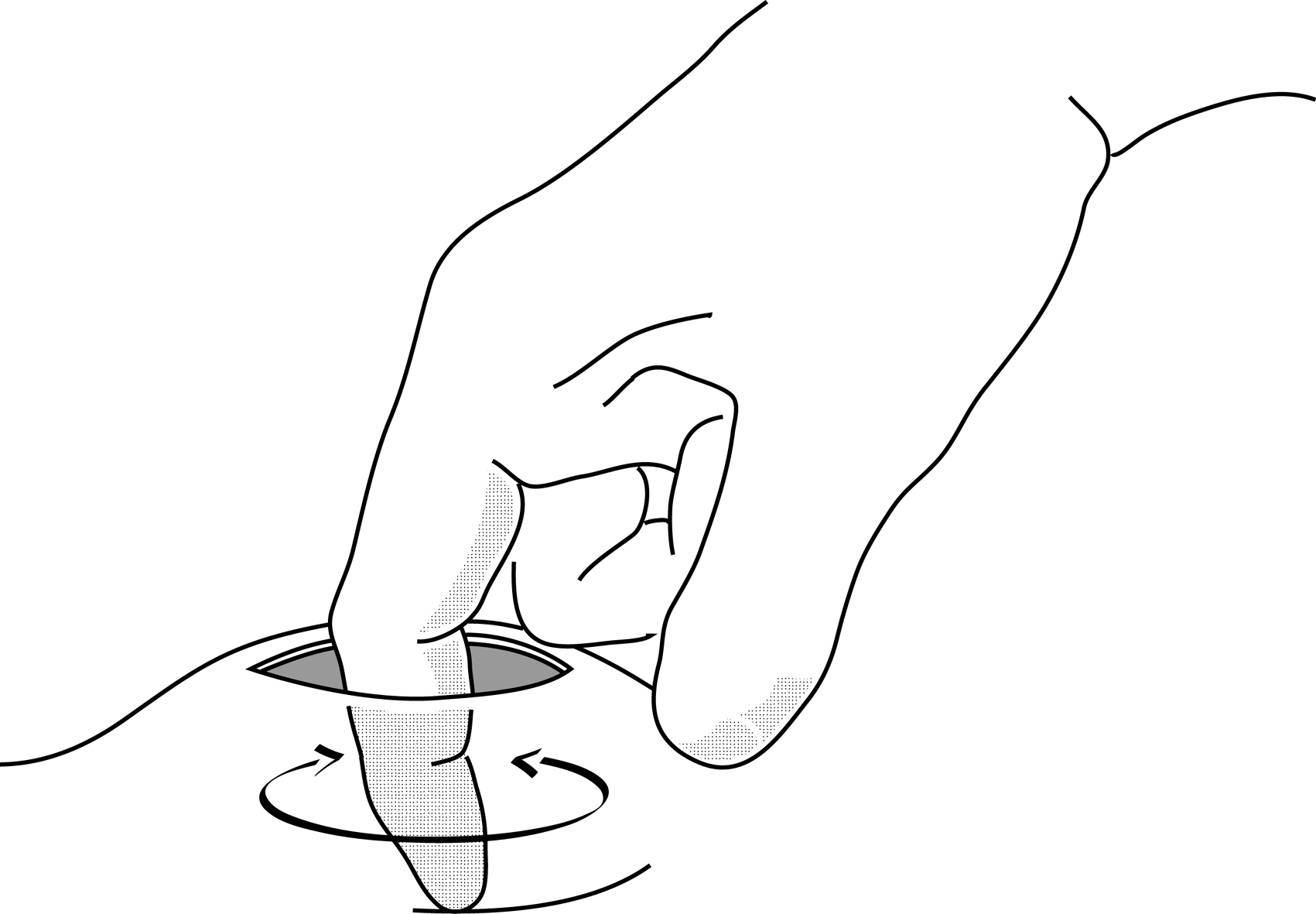
Figure 8b |
Washing
Abundant washing of the cavity using a syringe filled with 0.9% sodium chloride.
Drainage
(Figure 8c)
Only necessary for deep abscesses.
Insert a drain (or, failing that a gauze wick) into the base of the cavity. If possible, fix it to the edge of the incision with a single suture. The drain is withdrawn progressively and then, after 3 to 5 days removed completely.
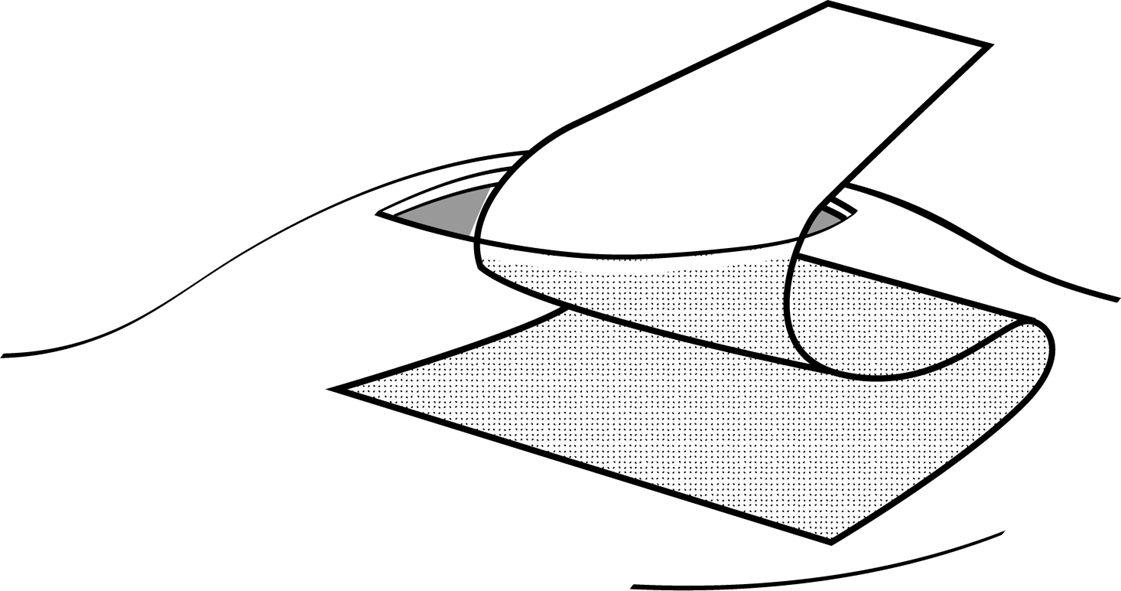
Figure 8c |
Dressing
Cover with sterile compresses.