Excessively prolonged active or pushing phase of labour. The term “prolonged labour” applies only at or after 5 cm dilation and 3 contractions per 10 minutes. Before that point, it is a “false labour” or prolonged latent phase.
Prolonged labour can be due to foeto-pelvic disproportion (mechanical dystocia) and/or inadequate contractions (dynamic dystocia) and/or ineffective maternal pushing efforts in the second stage of labour.
The main risks of prolonged labour are obstruction (Section 7.2) and foetal distress.
7.1.1 Diagnosis
- Arrest of cervical dilation for 4 hours during the active phase
or
- Protracted foetal engagement or descent after more than 2 hours of complete dilation in a multipara and 3 hours of complete dilation in a primipara
7.1.2 Management
See algorithms below.
For general patient care during labour, see Chapter 5, Section 5.1.4.
Notes:
- Oxytocin is contra-indicated in case of frank foeto-pelvic disproportion (risk of uterine rupture).
- In the event of foetal distress (baseline < 100/minute or deceleration > 5 minutes or repetitive decelerations after contraction for a period > 30 minutes)
aCitation a.In case a cardiotocograph is used, abnormal variability can also indicate foetal distress. For more information, see FIGO Intrapartum Fetal Monitoring Guidelines
https://www.figo.org/news/available-view-figo-intrapartum-fetal-monitoring-guidelines-0015088 and if the foetus is viable:- At complete dilation, with the presenting part engaged: instrumental delivery (Chapter 5, Section 5.6);
- Prior to complete dilation, or at complete dilation with presenting part not engaged: consider caesarean section earlier than in the algorithms, but the context needs to be taken into account when deciding a caesarean section for exclusive foetal indication (Chapter 6, Section 6.4).
In either case, do not use—or stop, if already using—oxytocin.
- If the foetus is dead, avoid caesarean section whenever possible. Allow more time for dilation and engagement. Consider embryotomy (Chapter 9, Section 9.7).
Management of arrest of cervical dilation for 4 hours during the active phase
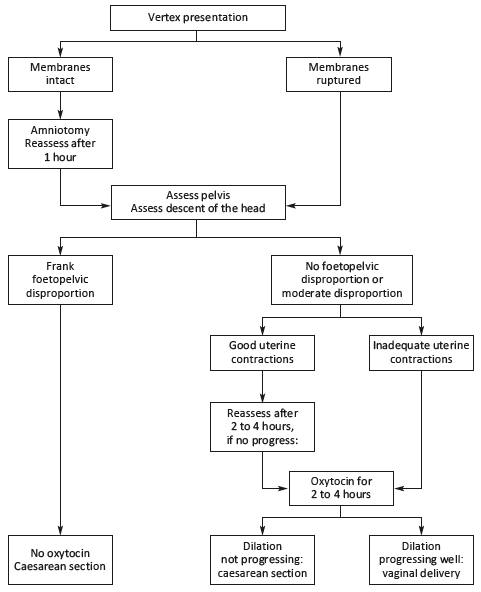
For other presentations, see breech presentation (Chapter 6, Section 6.1), transverse lie and shoulder presentation (Section 7.6), face presentation (Section 7.9), brow presentation (Section 7.10).
Management of protracted foetal engagement or descent after more than 2 hours of complete dilation in a multipara and 3 hours of complete dilation in a primipara
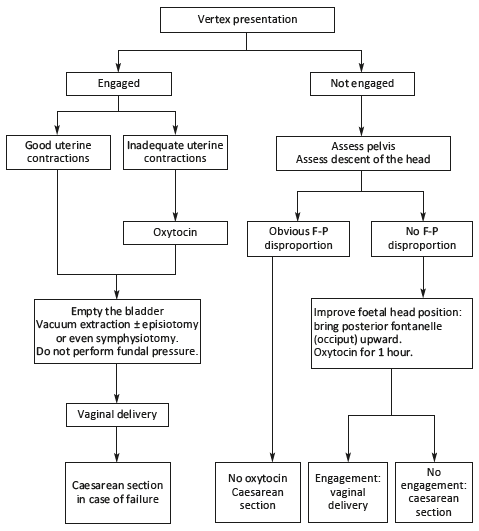
For other presentations (breech, shoulder, chin-posterior face, or brow presentations): caesarean section.
- (a)In case a cardiotocograph is used, abnormal variability can also indicate foetal distress. For more information, see FIGO Intrapartum Fetal Monitoring Guidelines
https://www.figo.org/news/available-view-figo-intrapartum-fetal-monitoring-guidelines-0015088