To avoid spreading the disease within the health care facility, devise a special circuit for patients suspected of having measles. As soon as they arrive, send suspect cases to a special waiting area that is separate from other patients, well-ventilated (if possible), and has its own dedicated care staff and equipment.
5.2.1 Diagnosis and sorting
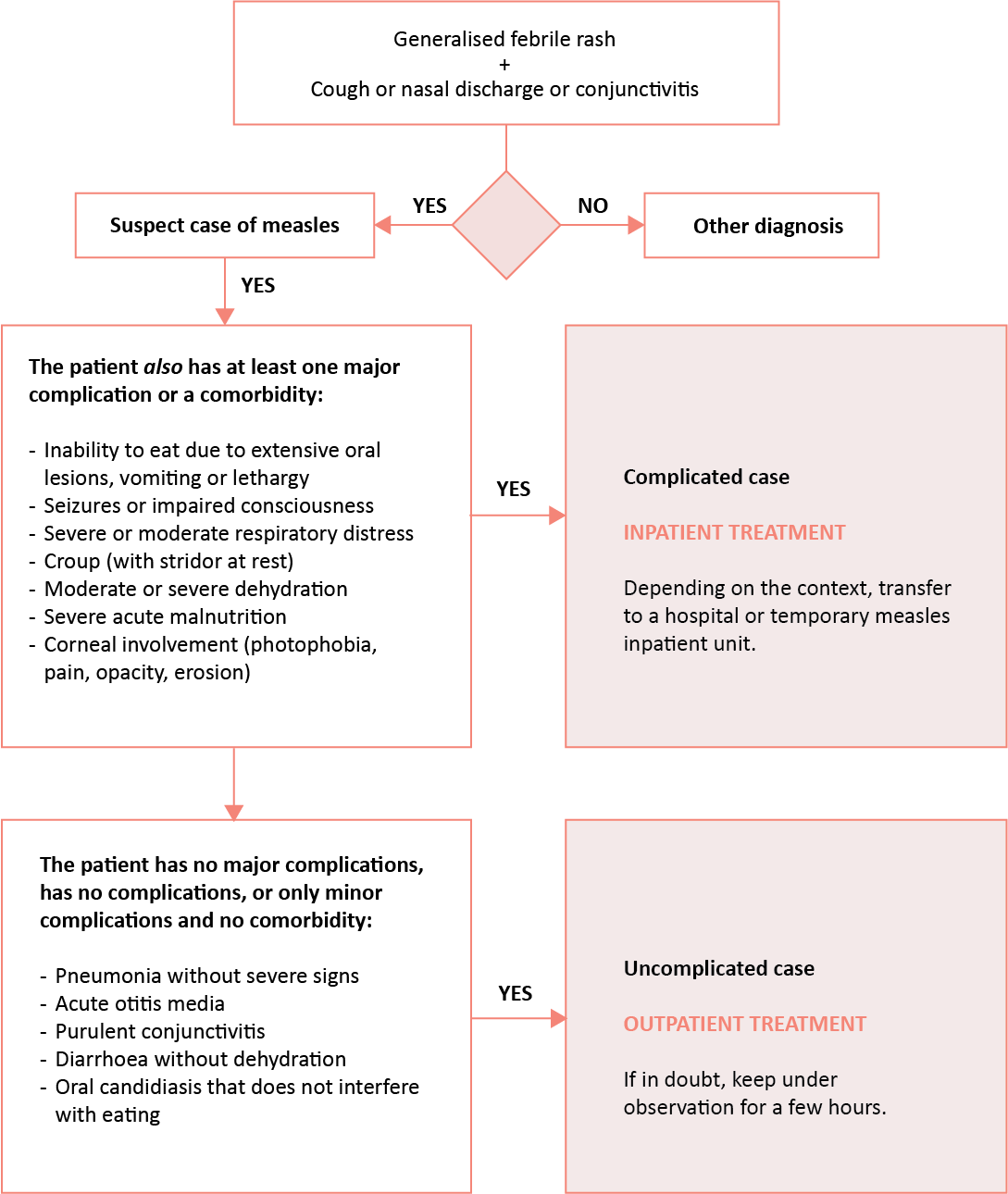
Look for clinical signs of measles and determine whether the patient is a “complicated case” or an “uncomplicated case”.
5.2.2 Initial clinical examination
[1]Citation 1.World Health Organization (WHO). Guide for Clinical Case Management and Infection Prevention and Control During a Measles Outbreak. Geneva: WHO; 2020.
https://www.who.int/publications/i/item/9789240002869
Establish the diagnosis
The diagnosis is based on clinical examination (see Section 5.1).
In practice, a suspected measles case is any patient with fever, a generalised maculopapular rash and at least one of the following signs: cough, runny nose or conjunctivitis.
Measure the axillary temperature or, at least, check if the child feels "hot”. The fever is generally high (> 39 °C).
Look for respiratory complications
- Check that the child is breathing normally, and not congested or dyspnoeic.
- Measure the respiratory rate (RR), especially if the child is coughing or dyspnoeic.
- If a clinician is present, auscultate the child to look for signs of pneumonia.
Decide whether to admit to inpatient unit using the criteria below:
| Pneumonia with no severe signs or comorbidities = DO NOT ADMIT TO INPATIENT UNIT | Severe pneumonia or with comorbidities = ADMIT TO INPATIENT UNIT |
|---|---|
| Fever and cough + Dyspnoea (high RR (a)Citation a.In children with severe malnutrition, the RR thresholds are 5 breaths/min lower. ) RR ≥ 60/min in a child under 2 months RR ≥ 50/min in a child from 2 to 11 months RR ≥ 40/min in a child from 1 to 5 years + Crackles on auscultation | Signs of pneumonia
|
Look for otitis
Look for ear pain and purulent discharge from the external auditory canal. Perform an otoscopic examination, if possible, depending on the examiner’s skill.
Otitis can be treated on an outpatient basis unless the child has other comorbidities
(= complicated case; see Section 5.4).
Look for ocular complications
Clean the eye if copious secretions interfere with the examination. Examine each eye separately, using a pen torch. Examine the conjunctiva and cornea. Determine whether or not there is corneal involvement. Proceed with care as corneal lesions are often painful and accompanied by photophobia (the patient shields their eyes from the light).
A normal cornea is transparent (it allows a clear view of the iris and pupil), moist, and shiny (it reflects the light). Any abnormality such as loss of transparency (opacity) or shininess (dull or dry cornea), or corneal softening (necrosis, perforation) is an indication for inpatient care
(= complicated case).
Purulent conjunctivitis alone (purulent discharge with discomfort or foreign body sensation, with no photophobia or corneal involvement) can be treated on an outpatient basis, unless the child is a “complicated case” for other reasons.
The examination may show Bitot’s spots. The child can be treated on an outpatient basis, unless other comorbidities are present (= complicated case; see Section 5.4).
Look for oral lesions
Oral candidiasis (white patches on the tongue or within the oral cavity) is considered benign unless it prevents the child from drinking and eating normally. It can be treated on an outpatient basis unless other comorbidities are present (= complicated case; see Section 5.4).
Painful or extensive lesions that prevent children from drinking or eating are considered severe (= complicated case) and require inpatient care.
Look for dehydration and/or diarrhoea
Always look for dehydration. Dehydration can have a number of causes, such as diarrhoea, insufficient fluid intake, repeated vomiting and high fever.
Whatever the cause, dehydrated patients must be admitted to inpatient care (= complicated case). |
Weight
Weigh the child whenever possible.
Ability to drink
Offer the child the breast or water to check they can drink properly; if the child cannot drink, keep under observation and hospitalise if the inability to drink persists.
Nutritional status
- Routinely check for acute malnutrition in children under 5 years using an anthropometric measurement and checking for bilateral lower extremity oedema.
- If there is bilateral oedema: acute malnutrition (= complicated measles case)
- If there is no bilateral oedema, measure the mid-upper arm circumference (MUAC):
- If MUAC ≥ 125 mm: the child is not malnourished
- If MUAC is between 115 and 124 mm: the child has moderate acute malnutrition
- If MUAC < 115 mm: the child has severe acute malnutrition (complicated measles case)
- In contexts where the weight-for-height (W/H) ratio is used:
- W/H ratio < -3Z: severe acute malnutrition (= complicated measles case)
Assess the carer’s ability to manage the patient and if they can return to the health facility with the child, if needed.
5.2.3 Additional tests
- Test for malaria in endemic areas.
- For complicated cases when equipment is available: O2 saturation, haemoglobin level, blood glucose in malnourished children, and chest X-ray (only for cases with respiratory signs).
- a
In children with severe malnutrition, the RR thresholds are 5 breaths/min lower.
- 1.
World Health Organization (WHO). Guide for Clinical Case Management and Infection Prevention and Control During a Measles Outbreak. Geneva: WHO; 2020.
https://www.who.int/publications/i/item/9789240002869