Measles is an extremely contagious acute viral infection, characterized by a fever and skin rash with signs of respiratory infection. It mainly affects children. There is no specific treatment for measles.
1.1.1 Scope of the problem
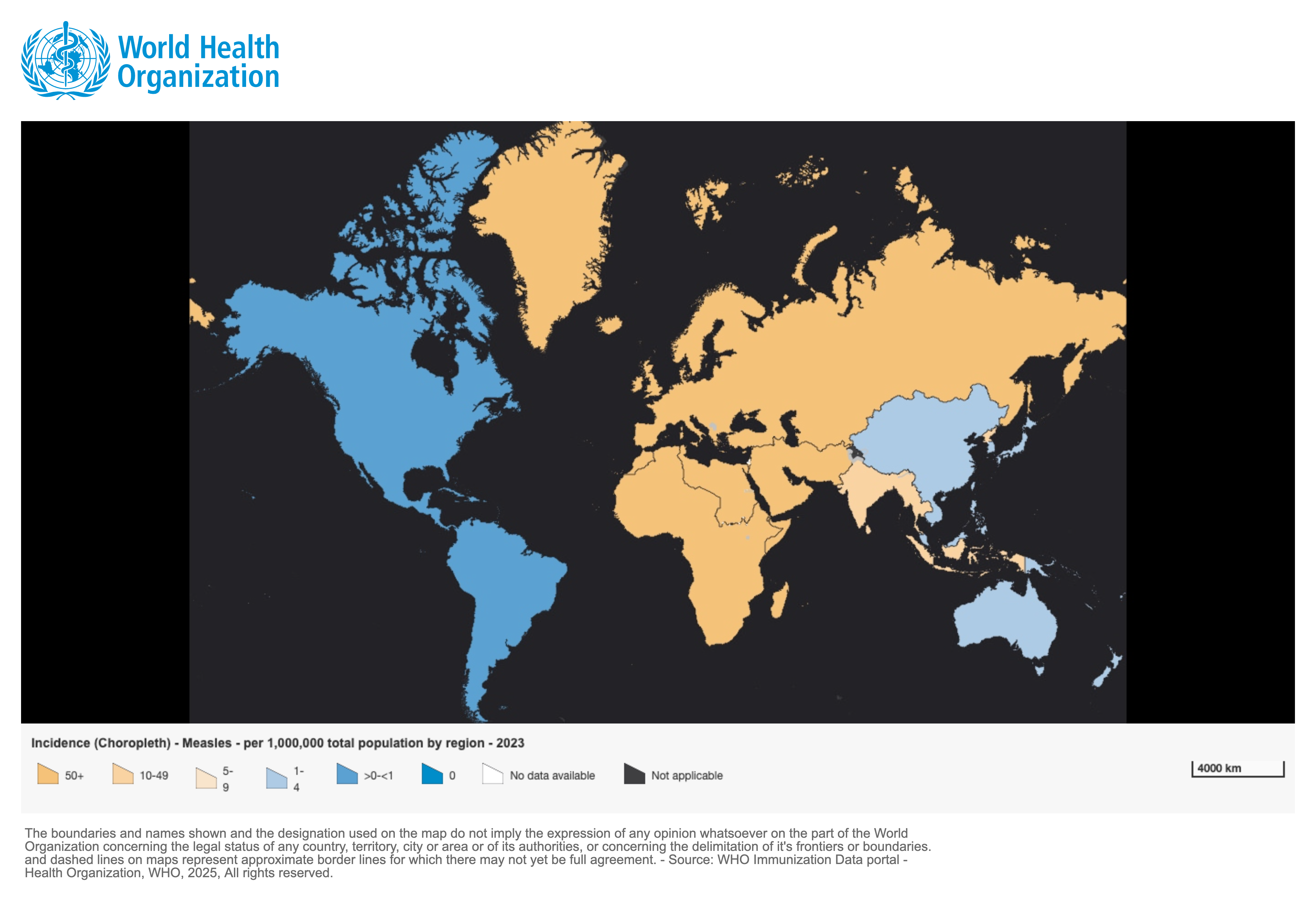
The introduction of an effective inexpensive vaccine in the 1960s helped reduce the scope of the disease on a global level. However, measles is still a major public health problem in countries where low vaccination coverage (in Africa and Asia, mainly) has allowed the disease to persist and give rise to large-scale outbreaks (Figure 1.1).
In 2023, 167 (out of 194) countries together reported 669,083 cases of measles
[1]Citation 1.Provisional monthly measles and rubella data. World Health Organization. Published March 2024. Available from:
https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/surveillance/monitoring/provisional-monthly-measles-and-rubella-data
. According to the WHO, despite overall improvements in epidemiological surveillance, these figures are probably still greatly underestimated
[1]Citation 1.Provisional monthly measles and rubella data. World Health Organization. Published March 2024. Available from:
https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/surveillance/monitoring/provisional-monthly-measles-and-rubella-data
.
Figure 1.1 - Incidence rate for reported measles cases per 100,000 people in 2023
[2]Citation 2.World Health Organization. Measles reported cases and incidence. Accessed March 29, 2025.
https://immunizationdata.who.int/global/wiise-detail-page/measles-reported-cases-and-incidence?CODE=Global&YEAR=
1.1.2 Infectious agent
Measles is caused by a paramyxovirus (morbillivirus), humans are the only reservoir (infected individuals, including those who are asymptomatic).
There are twenty-four currently known genotypes, divided into eight clades (designated by the letters A-H). Their distribution varies by region
[3]Citation 3.Measles. Centers for Disease Control and Prevention. Published 2019. Available from:
https://www.cdc.gov/measles/lab-tools/genetic-analysis.html, [4]Citation 4.Rota PA, Brown K, Mankertz A, et al. Global distribution of measles genotypes and measles molecular epidemiology. J Infect Dis. 2011;204(suppl_1):S514-S523.
https://doi.org/10.1093/infdis/jir118, [5]Citation 5.Broutin H, Mantilla-Beniers N, Simondon F, Aaby P, Grenfell BT, Guégan JF, Rohani P. Epidemiological impact of vaccination on the dynamics of two childhood diseases in rural Senegal. Microbes Infect. 2005;7(4):593-599. doi: 10.1016/j.micinf.2004.12.018
.
In endemic countries, most cases are caused by one or more geographically distributed endemic genotypes, with multiple co-circulating strains within the endemic genotype(s).
In regions where measles is well-controlled, the reintroduction of a case typically leads to outbreaks associated with a single virus genotype.
Molecular characterization of measles viruses allows for identifying their origin, monitoring their circulation, and detecting any genotype changes. It is essential for documenting the impact of global measles control programs.
1.1.3 Transmission
Transmission occurs primarily by direct contact with nasal or throat secretions by the airborne route.
Viral droplet nuclei shed by the infected individual infect the healthy individual by penetrating the nasal, oral, laryngeal or conjunctival mucosa. The virus can remain suspended in the air for more than two hours but does not survive long on objects or surfaces.
The contagious period begins three to four days before the rash appears and continues for up to five days after the rash begins. It can be longer in malnourished or immunodepressed individuals.
Measles is highly contagious. Its basic reproduction number, R0, is estimated to be between 12 and 18 (that is, one individual with acute measles can be the source of 12 to 18 secondary cases in a population where everyone is susceptible); that number can vary depending on the context (see Section 1.2.3).
1.1.4 Natural immunity
Immunity can be acquired naturally (by contracting the disease) or by vaccination.
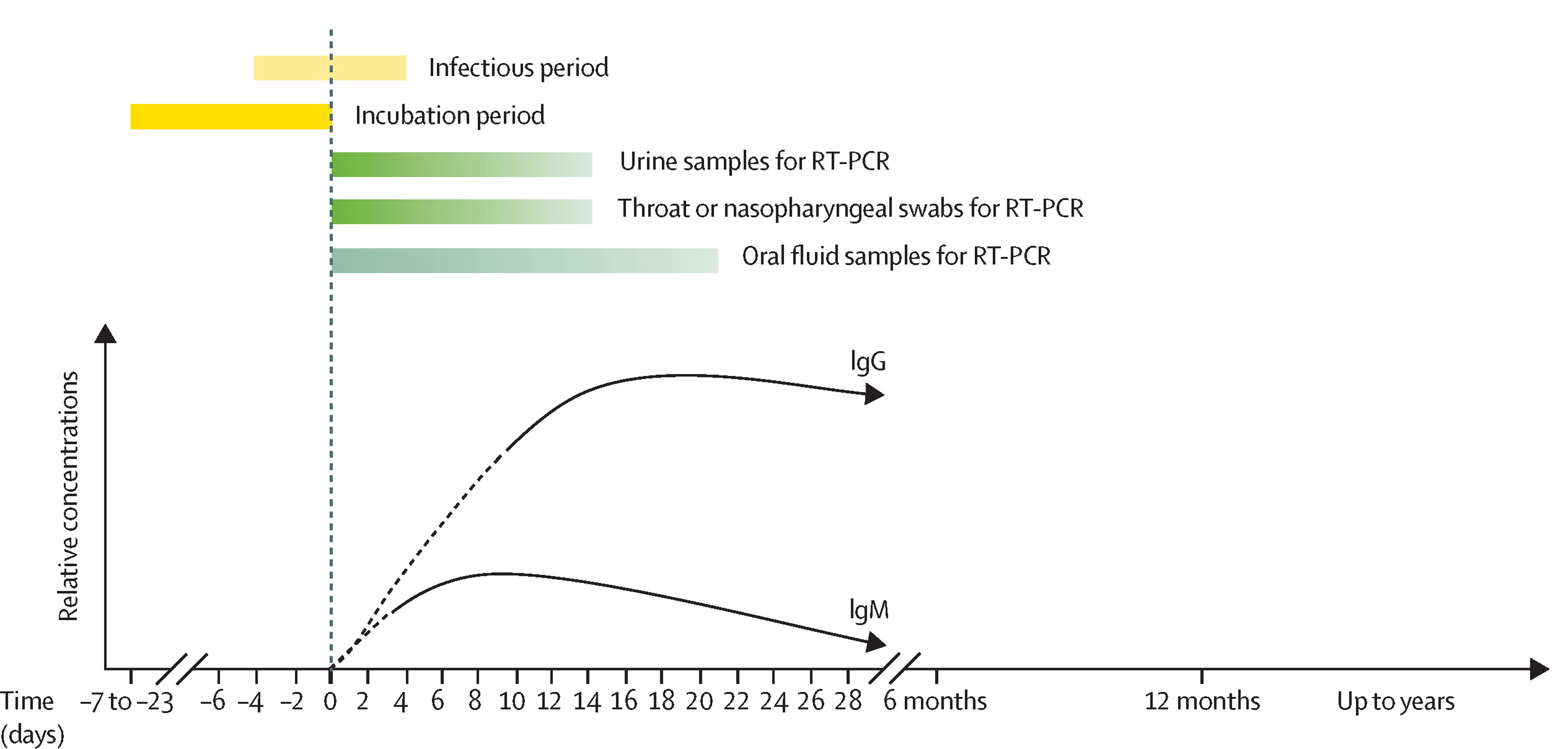
In infected individuals, immunoglobulin M (IgM) antibodies are detectable as soon as the rash appears and persist for about a month. Immunoglobulin G (IgG) antibodies appear a few days later and are detectable for life. Natural infection therefore confers lifelong protection.
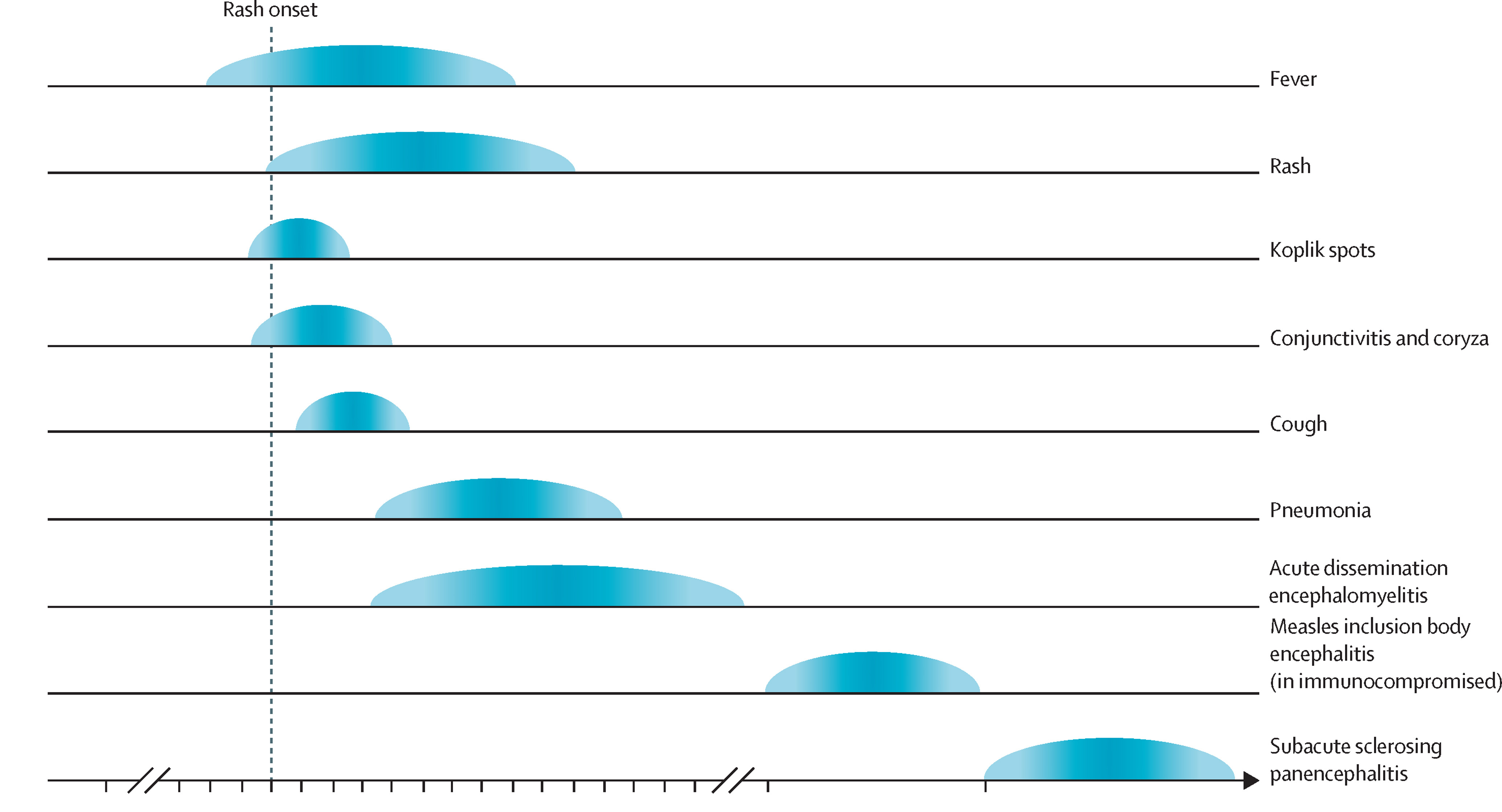
Figure 1.2 - Timeline of a typical measles infection and of some important complications [6]Citation 6.Hübschen JM, Gouandjika-Vasilache I, Dina J. Measles. Lancet. 2022;399(10325):678-690. https://doi.org/10.1016/S0140-6736(21)02004-3
During the illness, immune response activation helps eliminate the virus. Paradoxically, that activation causes the loss of pre-existing immunity to previously encountered pathogens
[7]Citation 7.Amurri L, Reynard O, Gerlier D, Horvat B, Iampietro M. Measles virus-induced host immunity and mechanisms of viral evasion. Viruses. 2022;14(12):2641.
doi: 10.3390/v14122641
, known as “immune amnesia
[8]Citation 8.Mina MJ, Kula T, Leng Y, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science. 2019;366(6465):599-606.
doi: 10.1126/science.aay6485
", leaving the patient susceptible to infection.
This primarily affects the memory lymphocytes, significantly reducing the antibody repertoire. The latter will then rebuild itself via exposure to infections and vaccination. This temporary deficit is significant for the first few months, but as time goes on the immune system re-establishes itself and patients regain their ability to defend themselves against other infections progressively over the next two to five years
[9]Citation 9.Gadroen K, Dodd CN, Masclee GMC, et al. Impact and longevity of measles-associated immune suppression: a matched cohort study using data from the THIN general practice database in the UK. BMJ Open. 2018;8(11):e021465.
doi: 10.1136/bmjopen-2017-021465
. Hence re-vaccinating for other diseases after measles appears necessary, but exactly how that should be done (number of doses, schedule, etc.) is still being studied.
Immune amnesia explains the long-observed and widely documented increase in post-measles morbidity and mortality
[7]Citation 7.Amurri L, Reynard O, Gerlier D, Horvat B, Iampietro M. Measles virus-induced host immunity and mechanisms of viral evasion. Viruses. 2022;14(12):2641.
doi: 10.3390/v14122641, [8]Citation 8.Mina MJ, Kula T, Leng Y, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science. 2019;366(6465):599-606.
doi: 10.1126/science.aay6485
.
It is important to note that the measles vaccine does not cause this phenomenon.
1.1.5 Vulnerability
Maternal antibodies, transmitted via the placenta and breast milk, protect infants for the first few months of life and then gradually disappear around age 6 to 9 months.
Once these antibodies have disappeared, all children become “susceptible,” that is, at risk of developing the disease if infected.
The age at which measles occurs is determined by the likelihood of contact with an individual that has measles. Vaccination coverage, birth rate, overcrowding, and population density are key factors.
Classically, in countries where the vaccination coverage is low and the birth rate is high, children under age 5 years– and more specifically those under age 3 years– are hit hardest; where vaccination coverage is higher, the average age of measles infection can shift toward adolescence and young adulthood.
A small percentage of vaccinated individuals will fail to develop immunity after the first dose of vaccine (5 to 15%, depending on age; see Chapter 2, Section 2.1.3). When vaccination is done at age 9 months, only 85% of children are protected and 15% are considered “non-responders,” hence the importance of a second dose later.
Without a second dose of the vaccine, these non-responders will always be at risk of developing the disease if infected.
1.1.6 Case fatality rate (CFR)
In industrialised countries, the case fatality rate is low, and the disease is often (wrongly) considered benign. The WHO estimates that in 2017, 3% of deaths in children under age 5 years worldwide were attributable to measles [10]Citation 10.Distribution of causes of death among children aged < 5 years (%). World Health Organization. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/distribution-of-causes-of-death-among-children-aged-5-years-(-) and that 90% of individuals who died from measles were younger than 5 years old. The delayed CFR due to post-measles complications and/or immune amnesia is probably higher but is rarely documented.
In a stable context, the CFR for measles in the community ranges from 1 to 5%, depending on the country’s health status, while the hospital CFR ranges from 1 to 10%
[11]Citation 11.Portnoy A, Jit M, Ferrari M, Hanson M, Brenzel L, Verguet S. Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(4):e472-e481.
https://doi.org/10.1016/s2214-109x(18)30537-0
.
The CFR is strongly dependent on:
Access to care: timeliness, distance to a healthcare facility, and how well simple and complicated cases are managed (admission criteria and quality of care). Rural areas with poor access to care are therefore at risk of a high CFR [12]Citation 12.Gignoux E, Polonsky J, Ciglenecki I, et al. Risk factors for measles mortality and the importance of decentralized case management during an unusually large measles epidemic in eastern Democratic Republic of Congo in 2013. In: Arez AP, ed. PLoS One. 2018;13(3):e0194276. doi: 10.1371/journal.pone.0194276 .
Population density: areas with high population density like poor urban areas (slums) and IDP and refugee camps, which are conducive to high viral exposure, are also at risk of a high CFR [13]Citation 13.Aaby P, Bukh J, Lisse IM, Smits AJ. Overcrowding and intensive exposure as determinants of measles mortality. Am J Epidemiol. 1984;120(1):49-63. doi: 10.1093/oxfordjournals.aje.a113874 .
Family size (the more children, the higher the risk) [14]Citation 14.Sbarra AN, Jit M, Mosser JF, et al. Population-level risk factors related to measles case fatality: a conceptual framework based on expert consultation and literature review. Vaccines. 2023;11(8):1389. doi: 10.3390/vaccines11081389 .
At the individual level, the main aggravating factors are:
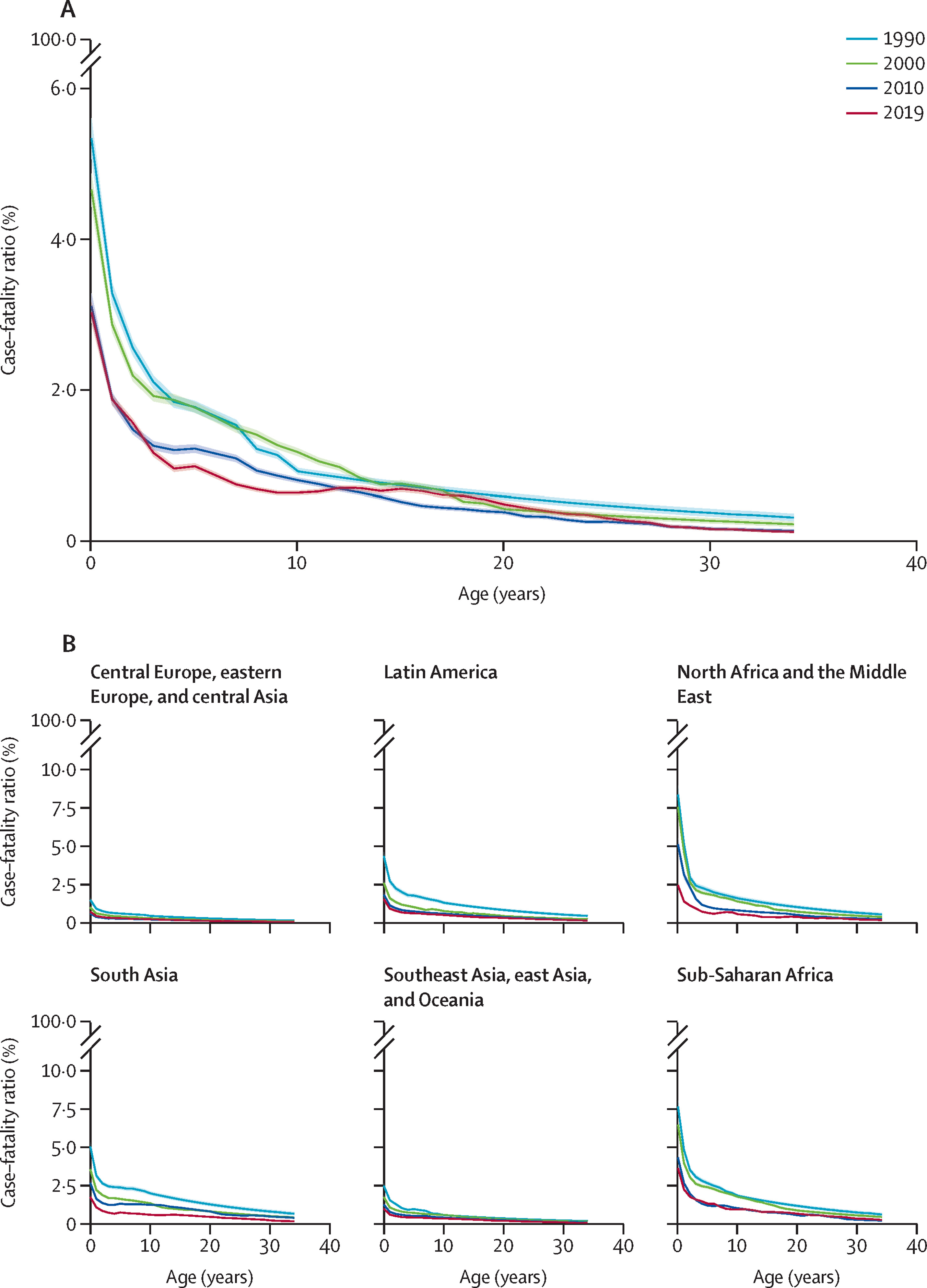
Age: the CFR is high among young children, particularly if the quality of care is limited, and gradually declines with age (see Figure 1.3)
Acute or chronic malnutrition
Vitamin A deficiency
Not being vaccinated against measles
Immune deficiency and, in particular, HIV coinfection [15]Citation 15.Sbarra AN, Jit M, Mosser JF, et al. Population-level risk factors related to measles case fatality: a conceptual framework based on expert consultation and literature review. Vaccines. 2023;11(8):1389. Available from: https://doi.org/10.3390/vaccines11081389 .
Figure 1.3 (A) - Estimated case fatality rate for measles by age (in years) for 1990, 2000, 2010 and 2019 and Figure 1.4 (B) – Estimated case fatality rate for measles by WHO subregion for 1990, 2000, 2010 and 2019 [16]Citation 16.Sbarra AN, Mosser JF, Jit M, Ferrari M, Ramshaw RE, O’Connor P, et al. Estimating national-level measles case–fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study. The Lancet Global Health [Internet]. 2023 Apr 1;11(4):e516–24. Available from: https://www.sciencedirect.com/science/article/pii/S2214109X23000438
- 1.
Provisional monthly measles and rubella data. World Health Organization. Published March 2024. Available from:
https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/surveillance/monitoring/provisional-monthly-measles-and-rubella-data
- 2.
World Health Organization. Measles reported cases and incidence. Accessed March 29, 2025.
https://immunizationdata.who.int/global/wiise-detail-page/measles-reported-cases-and-incidence?CODE=Global&YEAR= - 3.
Measles. Centers for Disease Control and Prevention. Published 2019. Available from:
https://www.cdc.gov/measles/lab-tools/genetic-analysis.html - 4.
Rota PA, Brown K, Mankertz A, et al. Global distribution of measles genotypes and measles molecular epidemiology. J Infect Dis. 2011;204(suppl_1):S514-S523.
https://doi.org/10.1093/infdis/jir118 - 5.
Broutin H, Mantilla-Beniers N, Simondon F, Aaby P, Grenfell BT, Guégan JF, Rohani P. Epidemiological impact of vaccination on the dynamics of two childhood diseases in rural Senegal. Microbes Infect. 2005;7(4):593-599. doi: 10.1016/j.micinf.2004.12.018
- 6.
Hübschen JM, Gouandjika-Vasilache I, Dina J. Measles. Lancet. 2022;399(10325):678-690. https://doi.org/10.1016/S0140-6736(21)02004-3
- 7.
Amurri L, Reynard O, Gerlier D, Horvat B, Iampietro M. Measles virus-induced host immunity and mechanisms of viral evasion. Viruses. 2022;14(12):2641.
doi: 10.3390/v14122641 - 8.
Mina MJ, Kula T, Leng Y, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science. 2019;366(6465):599-606.
doi: 10.1126/science.aay6485 - 9.
Gadroen K, Dodd CN, Masclee GMC, et al. Impact and longevity of measles-associated immune suppression: a matched cohort study using data from the THIN general practice database in the UK. BMJ Open. 2018;8(11):e021465.
doi: 10.1136/bmjopen-2017-021465 - 10.
Distribution of causes of death among children aged < 5 years (%). World Health Organization. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/distribution-of-causes-of-death-among-children-aged-5-years-(-)
- 11.
Portnoy A, Jit M, Ferrari M, Hanson M, Brenzel L, Verguet S. Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(4):e472-e481.
https://doi.org/10.1016/s2214-109x(18)30537-0 - 12.
Gignoux E, Polonsky J, Ciglenecki I, et al. Risk factors for measles mortality and the importance of decentralized case management during an unusually large measles epidemic in eastern Democratic Republic of Congo in 2013. In: Arez AP, ed. PLoS One. 2018;13(3):e0194276. doi: 10.1371/journal.pone.0194276
- 13.
Aaby P, Bukh J, Lisse IM, Smits AJ. Overcrowding and intensive exposure as determinants of measles mortality. Am J Epidemiol. 1984;120(1):49-63. doi: 10.1093/oxfordjournals.aje.a113874
- 14.
Sbarra AN, Jit M, Mosser JF, et al. Population-level risk factors related to measles case fatality: a conceptual framework based on expert consultation and literature review. Vaccines. 2023;11(8):1389. doi: 10.3390/vaccines11081389
- 15.
Sbarra AN, Jit M, Mosser JF, et al. Population-level risk factors related to measles case fatality: a conceptual framework based on expert consultation and literature review. Vaccines. 2023;11(8):1389. Available from: https://doi.org/10.3390/vaccines11081389
- 16.
Sbarra AN, Mosser JF, Jit M, Ferrari M, Ramshaw RE, O’Connor P, et al. Estimating national-level measles case–fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study. The Lancet Global Health [Internet]. 2023 Apr 1;11(4):e516–24. Available from: https://www.sciencedirect.com/science/article/pii/S2214109X23000438