The outbreak situation needs to be assessed for several weeks after the vaccination campaign ends. This assessment includes the following steps (which, depending on the resources, can be conducted in parallel):
- Post-vaccination campaign case surveillance and continued awareness-raising and patient care activities
- Identification of any problems encountered during the campaign
- Vaccination coverage evaluation (population survey)
- Catch-up activities
- Vaccine effectiveness, if in doubt
7.6.1 Continued case surveillance, patient care and awareness-raising
It is important to continue to monitor for new cases in the weeks after the vaccination campaign. Some vaccine side effects can (temporarily) resemble symptoms of the disease (false positives), and children continue to be vulnerable for at least two weeks after vaccination (the time it takes to develop effective immunity).
After that, strict surveillance makes it possible to anticipate and quickly respond to any new outbreaks, especially if administrative coverage during the campaign was found to be suboptimal. Every new suspected case requires rapid laboratory confirmation and treatment.
It is also important to continue community awareness activities to reassure parents about vaccine side effects and stress the continued importance of bringing children in if they suspect measles and the need to continue routine vaccination according to the immunisation schedule.
7.6.2 Analysis of the campaign’s effectiveness
Failure to see a drop in cases two weeks after the campaign should prompt the following questions about the campaign’s operation:
- Were there any problems during the vaccination campaign?
Have barriers to vaccination that might explain inadequate coverage already been identified and resolved, at least in part? (See section 7.3) If so, quickly schedule appropriate catch-up activities.
- Opt for a vaccination coverage survey (population survey)
A post-campaign vaccination coverage survey in the target population is often helpful in assessing its impact. In particular, design permitting, it provides a detailed mapping of low-coverage pockets and an understanding of the local geographic, social, and operational determinants, allowing targeted responses.
Principle:
While measles vaccination campaigns are a key component in fighting measles outbreaks, they are only effective if vaccination coverage is high enough.
An evaluation of vaccination coverage measures the proportion of the target population that has been vaccinated and identifies non-vaccinated groups (age groups and specific populations like remote villages, IDPs and refugees not included in the planning).
Objectives
The survey should, at a minimum, answer the following questions:
- Did these people arrive at the vaccination area just recently (new arrivals, refugees/IDPs) and so could not be vaccinated?
- Are there geographic “pockets” of non-vaccinated people or is coverage low everywhere?
- What are the reasons for non-vaccination?
Using the results
If the estimated VC is close to 100% after analysing the results, consider the vaccination campaign effective and successful. If that is not the case, identify the groups or geographic areas where coverage is below the herd immunity threshold for measles and the reasons for non-vaccination and use that information to adapt and target awareness-raising activities and vaccination catch-up activities.
Vaccination coverage surveys are generally conducted by an epidemiologist and a dedicated team; they can be expensive in terms of resources and usually take one to three weeks, depending on the size of the targeted area.
Consider a vaccination effectiveness study:
- If the surveillance system continues to report suspected cases weeks after the campaign (even after any catch-up activities guided by the vaccination coverage survey), make sure that they are indeed measles cases (review the case definitions and get laboratory confirmation), since measles can easily be confused with rubella.
- Otherwise:
- If the survey shows VC ≥ 80% AND
- There is laboratory confirmation that they are indeed measles cases AND
- The mass vaccination campaign went smoothly and the coverage survey confirms good administrative vaccination coverage, consider a vaccine effectiveness study.
Definition of vaccine effectiveness
It’s important to distinguish between vaccine efficacy (the intrinsic immunogenicity of the vaccine) as measured under controlled randomised clinical trial conditions and the vaccine’s actual effectiveness as observed during large-scale use in the general population. This real-world effectiveness includes not just the performance of the vaccine itself, but also the impact of multiple factors such as the age of the subjects being vaccinated, their underlying immunological status, and potential programme-related errors (e.g. cold chain failures, reconstitution/administration problems, etc.).
When is it measured?
There are several situations in which effectiveness in the field needs to be evaluated: when outbreaks occur in correctly-vaccinated populations with high vaccination coverage (measured); when there is no reduction in measles incidence despite high vaccination coverage; when a significant percentage of the reported cases had already been vaccinated; and when a new vaccine is introduced.
The principle is based on a calculation of the percentage reduction in the attack rate (or risk of contracting the disease) among the vaccinated compared to the rate among unvaccinated people exposed to the same risk.
How is it measured?
Different study designs with varying degrees of complexity and robustness can be used to measure effectiveness under real world conditions.
Rapid estimation method: the screening method
This method is most appropriate in operational situations because it only requires programmatic vaccination coverage data (percentage of the population vaccinated, or PPV, using coverage surveys, if possible) and the percentage of cases vaccinated (PCV).
The formula is: VE (in %) = (PPV – PCV) / [PPV x (1-PCV)]
While easy to use, this method yields only a biased approximation of the effectiveness, and its reliability is strongly dependent on the quality of the data collected.
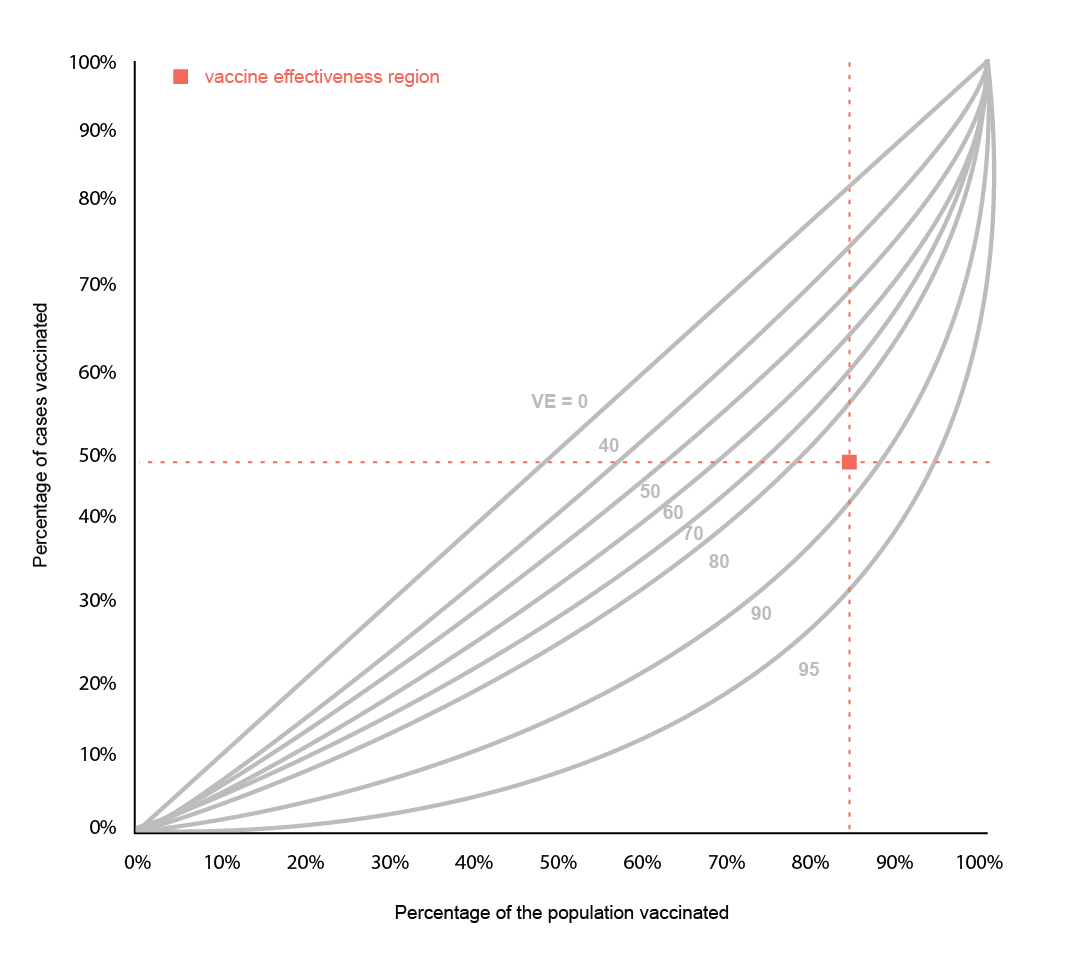
Screening method example
A vaccination campaign was conducted 9 months ago. A vaccination coverage survey showed that 85% of the target population was vaccinated (PPV = 85%).
Some measles cases have been reported; half of them were vaccinated during the campaign (PCV = 50%).
EV = [0.85 - 0.50] / 0.8 x (1 - 0.5) = [0.35] / (0.425) = 82%
Drawing a straight vertical line from 85% on the x-axis and a straight horizontal line from 50% on the y-axis, the two lines intersect in the vaccine effectiveness region between the 0.8 and the 0.9 curves, consistent with the value obtained by calculation.
Figure 7.1 - Nomogram
More complicated methods
The following methods are more rigorous and reliable but require epidemiological expertise (contact your vaccination advisor).
Prospective cohort surveys, case-control studies, and so-called “test negative” studies allow calculation of vaccine effectiveness by comparing the attack rates between the vaccinated and unvaccinated, adjusting for any confounders. These studies are expensive and difficult to set up.
Validity and reliability of the results
Whichever method is used, valid, reliable results will require:
- A standardised, consistently-applied case definition
- An exhaustive search for and rigorous identification of all cases in the population of interest
- Accurate determination of actual vaccination status (preferably by presentation of an immunisation record)
- Comparable risk of disease exposure between the vaccinated and unvaccinated groups being studied
The study sample should be representative of all of the measles cases that have occurred in the geographic area being evaluated.