Genital ulcers, defined as single or multiple vesicular, ulcerative or erosive lesions of the genital tract, with or without inguinal lymphadenopathy, should lead to consideration of sexually transmitted infection.
The principal causative organisms are Treponema pallidum (syphilis), Haemophilus ducreyi (chancroid) and Herpes simplex (genital herpes). Chlamydia trachomatis (lymphogranuloma venereum) and Calymmatobacterium granulomatis (donovanosis) aCitation a.Lymphogranuloma venereum is endemic in East and West Africa, India, Southeast Asia, South America and the Caribbean. Donovanosis is endemic in South Africa, Papua New Guinea, India, Brazil and the Caribbean. are less frequent.
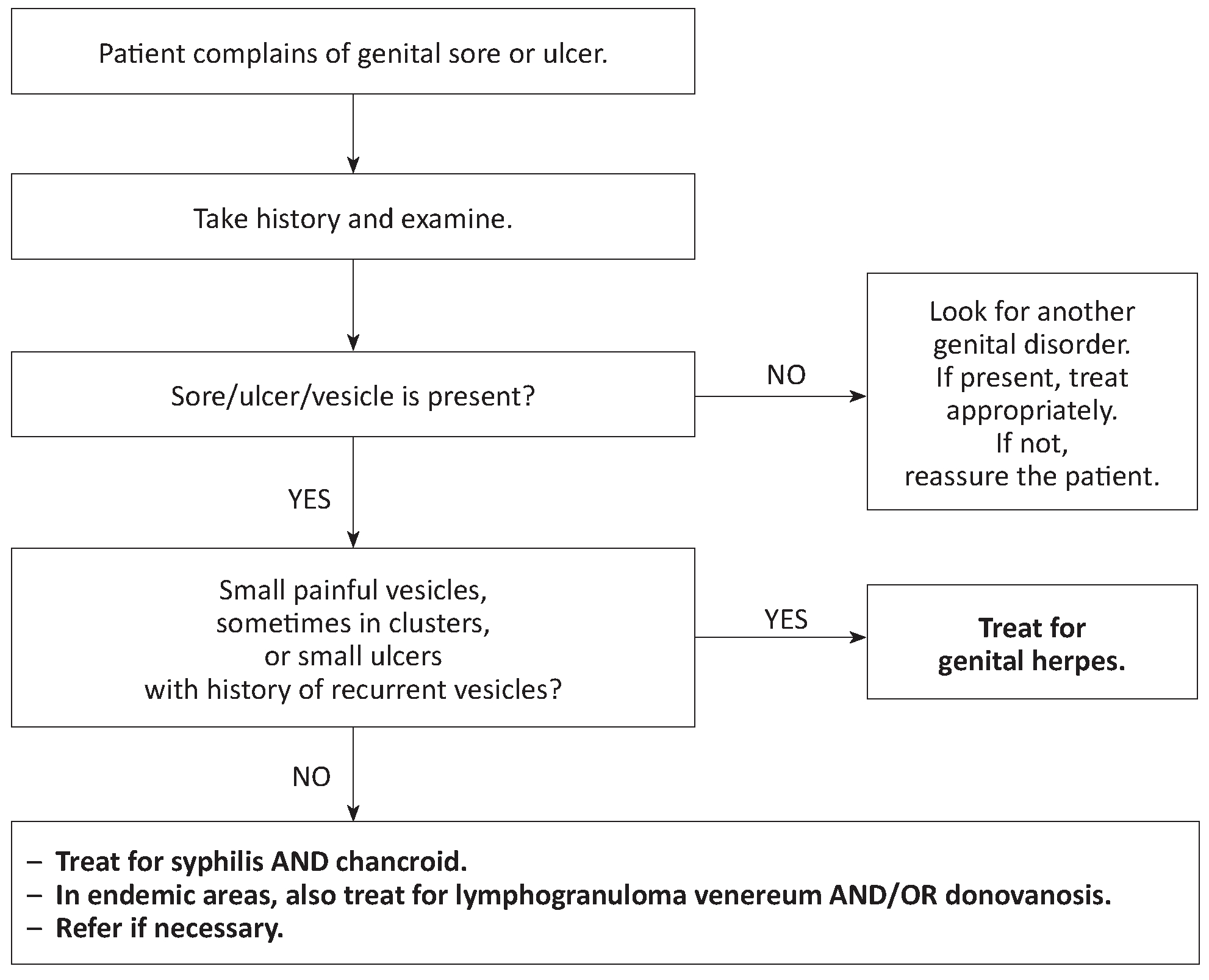
Case management
Laboratory
Laboratory testing available in the field is of little value: e.g., in syphilis, a negative RPR or VDRL result does not exclude primary syphilis in early stage, and a positive test may reflect previous infection in a successfully treated patient.
Treatment of the patient
Genital herpes
- Local treatment: clean the area with soap and water.
- Antiviral treatment: aciclovir PO
In patients with a first episode, treatment may reduce the duration of symptoms when given within 5 days after the onset of symptoms: 400 mg 3 times daily for 7 days.
In patients with recurrence, give the same dose for 5 days, but treatment is only effective if initiated during the prodromal phase or within 24 hours after the onset of symptoms.
In patients with frequent recurrences (more than 6 episodes par year).
- Treatment of pain: paracetamol PO (Chapter 1).
Syphilis
benzathine benzylpenicillin IM: 2.4 MUI per injection (half the dose in each buttock)
[1]Citation 1.Centers for Disease Control and Prevention. Syphilis Pocket Guide for Providers. 2017.
https://www.cdc.gov/std/syphilis/Syphilis-Pocket-Guide-FINAL-508.pdf
.
Early syphilis (primary, secondary, or early latent infection of less than 12 months duration): single dose
Late latent syphilis (infection of more than 12 months duration or of unknown duration): one injection weekly for 3 weeks
or, for penicillin-allergic patients or if penicillin is not available:
erythromycin PO: 1 g 2 times daily or 500 mg 4 times daily for 14 days (early syphilis) or 30 days (late latent syphilis)
or
doxycycline PO: 100 mg 2 times daily for 14 days (early syphilis) or 30 days (late latent syphilis)
bCitation b.Doxycycline is contra-indicated in pregnant and breast-feeding women.
or
azithromycin PO: 2 g single dose (only in cases of early syphilis and only if the strain is sensitive)
[2]Citation 2.World Health Organization. WHO guidelines for the treatment of Treponema pallidum (syphilis), Geneva, 2016.
http://apps.who.int/iris/bitstream/handle/10665/249572/9789241549806-eng.pdf?sequence=1
Chancroid
azithromycin PO: 1 g single dose
or
ceftriaxone IM: 250 mg single dose
or
erythromycin PO: 1 g 2 times daily or 500 mg 4 times daily for 7 days
Fluctuant lymph nodes may be aspirated through healthy skin as required. Do not incise and drain lymph nodes.
Note: treat simultaneously for syphilis AND chancroid as both are frequent, and cannot be correctly distinguished on clinical grounds.
Lymphogranuloma venereum
erythromycin PO: 1 g 2 times daily or 500 mg 4 times daily for 14 days
or
doxycycline PO: 100 mg 2 times daily for 14 days
bCitation b.Doxycycline is contra-indicated in pregnant and breast-feeding women.
Fluctuant lymph nodes may be aspirated through healthy skin as required. Do not incise and drain lymph nodes.
Donovanosis
Treatment is given until the complete disappearance of the lesions (usually, several weeks; otherwise risk of recurrence):
azithromycin PO: 1 g on D1 then 500 mg once daily
or
erythromycin PO: 1 g 2 times daily or 500 mg 4 times daily
or
doxycycline PO: 100 mg 2 times daily
bCitation b.Doxycycline is contra-indicated in pregnant and breast-feeding women.
In HIV infected patients, add gentamicin IM: 6 mg/kg once daily.
Treatment of the partner
The sexual partner receives the same treatment as the patient, whether or not symptoms are present, except in the case of genital herpes (the partner is treated only if symptomatic).
- 1.Centers for Disease Control and Prevention. Syphilis Pocket Guide for Providers. 2017.
https://www.cdc.gov/std/syphilis/Syphilis-Pocket-Guide-FINAL-508.pdf - 2.World Health Organization. WHO guidelines for the treatment of Treponema pallidum (syphilis), Geneva, 2016.
http://apps.who.int/iris/bitstream/handle/10665/249572/9789241549806-eng.pdf?sequence=1