On this page
Tears occur during delivery, and are more common in cases of cervical oedema, large foetus, or instrumental extraction (forceps or vacuum extractor).
A special sterile set containing vaginal retractors and long instruments should be available in every maternity ward for exploration and treatment of deep cervical and vaginal tears.
8.5.1 Diagnosis
Suspect a tear in cases of postpartum haemorrhage where there is good uterine retraction and uterine rupture has been ruled out.
The source of the bleeding is discovered during inspection of the birth canal, with careful examination of the vagina and cervix using two vaginal retractors.
8.5.2 Management
- Insert an IV line (16-18G catheter) and administer Ringer lactate or 0.9% sodium chloride.
- In the event of blood loss > 500 ml, see Section 8.2.
- If possible, perform spinal or general anaesthesia to get good exposure.
- An assistant is usually needed to present the tissues using retractors. Good lighting is essential.
- Swab the perineum with 10% povidone iodine.
- Gently pull the cervix toward the outside using atraumatic forceps (ring forceps, for example) and assess the extent of the tears:
- Small cervical tear, minimal bleeding: should heal spontaneously with no suturing and without complications.
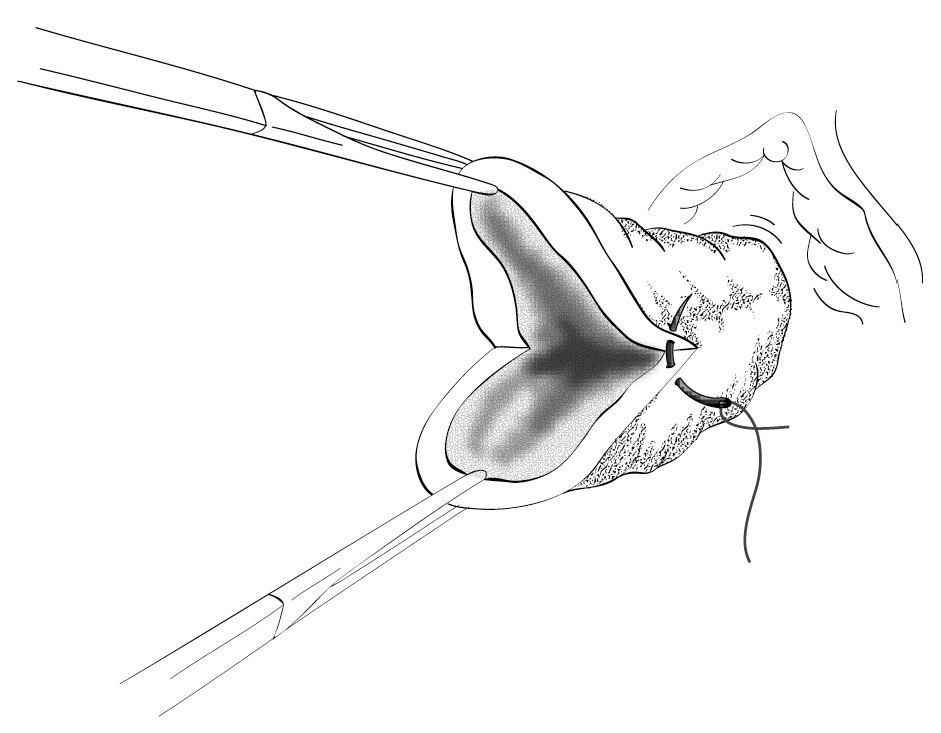
- Larger cervical tear, heavy bleeding: a few Dec 3 (2-0) absorbable figure-of-eight sutures in a single layer. Place the initial suture above the apex of laceration to control retracted arteries (Figure 8.8).
- The vaginal walls should also be sutured in the event of a bleeding laceration. For multiple vaginal lacerations with friable tissue that tears on suturing, insert a vaginal pack and remove after 24 hours. Insert a Foley catheter while the pack is in place.
- If the tear extends up to the uterus (lower segment), transfer the patient to a surgical setting for laparotomy.
Figure 8.8 - Cervical tear