The third stage of labour refers to the period that starts immediately after delivery of the infant and ends with the completed delivery of the placenta and its attached membranes.
There is a significant risk of haemorrhage during this stage. All patients require close monitoring and routine prevention of postpartum haemorrhage (PPH).
8.1.1 Description
This stage usually lasts 5 to 15 minutes.
- After the infant is delivered, there is a rest period without contractions that lasts, on average, 10 minutes. Use this time to take care of the neonate. Watch the mother carefully, however, for signs of PPH, which can occur at any time.
- Then, contractions resume, the placenta separates spontaneously. On abdominal palpation the uterine fundus can be felt ascending and then descending again, corresponding to the migration/descent of the placenta. When the entire placenta has reached the vagina, the uterus retracts and forms a hard ball above the pubic bone.
- The blood loss accompanying delivery of the placenta should not exceed 500 ml.
In the absence of PPH, a maximum delay of 30 to 45 minutes is tolerated for the expulsion of the placenta. After that, the placenta should be removed manually (Chapter 9, Section 9.2).
8.1.2 Routine prevention of postpartum haemorrhage
Active management of third stage of labour
Active management of third stage of labour consists in the administration of oxytocin before placental expulsion, followed by controlled cord traction then uterine massage to help retraction of the uterus.
After the birth, palpate the mother's abdomen to be sure she is not carrying twins. Administration of 5 or 10 IU oxytocin slow IV or IM immediately after the birth (after the birth of the last infant in a multiple pregnancy) AND before delivery of the placenta accelerates separation of the placenta, facilitates its delivery and helps prevent PPH.
Then, after clamping and cutting the cord, deliver the placenta with controlled cord traction (during a contraction with counter pressure to the uterus, with a hand placed on the abdomen). Uncontrolled traction on the cord (i.e., done without a contraction or counterpressure) is contra-indicated, as it can cause tearing of the placenta and, afterwards, retention of placental fragments with risk of bleeding and infection.
When oxytocin is used prior to placental delivery, there is, in theory, and especially if the injection is not done immediately (i.e. within 3 minutes), a risk of retained placenta. For this reason, the birth attendant who administers oxytocin immediately after birth must be able to perform manual removal of the placenta, should it be necessary. If these conditions are not met, oxytocin should be administered after placental expulsion.
Administration of oxytocin after placental delivery
If oxytocin has not been given prior to placental delivery, it should be administered after the placenta has been completely delivered. However, this is less effective in preventing PPH.
oxytocin slow IV or IM: 5 or 10 IU
Uterine exploration to remove any placental fragments will be more difficult after injecting oxytocin. Be sure that the placenta is complete before administering oxytocin.
In addition, massage the uterus to help uterine retraction.
8.1.3 Monitoring
- Heart rate, blood pressure, the amount of blood loss, while waiting for the placenta to deliver and after placental expulsion (every 15 minutes for the first hour, then every 30 minutes for the next hour) as the risk of PPH persists.
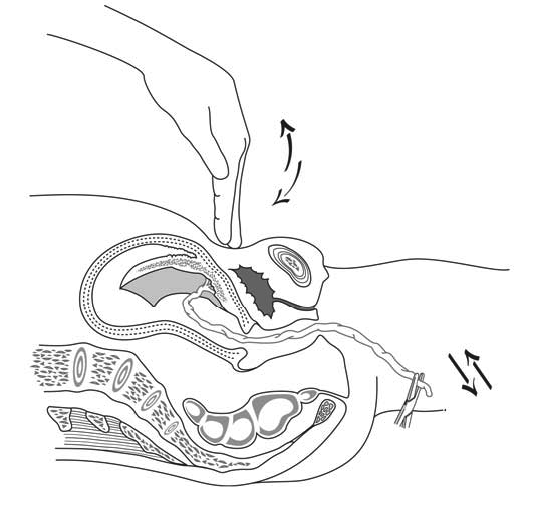
- Placental separation: press down on the abdomen just above the pubic bone. If the cord does not retract when pressure is applied, the placenta has separated (Figure 8.1). To facilitate expulsion from the vagina if it seems to be going slowly after the separation, apply moderate pressure to the uterine fundus, directed toward the vagina.
- The uterus retracts and remains retracted.
Figure 8.1 - Placental separation has occurred if the cord fails to retract with abdominal pressure
8.1.4 Examination of the placenta
Examine the placenta to verify that it has been completely expelled. The uterus can only retract properly if it is empty. Sooner or later, retained debris will lead to haemorrhage or infection.
Examination of the membranous sac
Straighten the sac by inserting a hand into it, looking for a vessel that ends abruptly— indicating that there might be a succenturiate lobe remaining in the uterus—or for a tear pointing to retained membrane. In these cases, manual uterine exploration may be required (Chapter 9, Section 9.3).
Examination of the maternal surface of the placenta
Regular, bright red cotyledons. Any holes, roughened or depressed areas, or any deep cuts that fail to line up when the cotyledons are brought together may suggest retained placenta, requiring uterine exploration.