On this page
The umbilical cord drops in front of the presenting part, usually when the membranes rupture (due to low insertion or excessive length, transverse or breech presentation, sudden rupture of the amniotic sac, excess amniotic fluid, twin pregnancy).
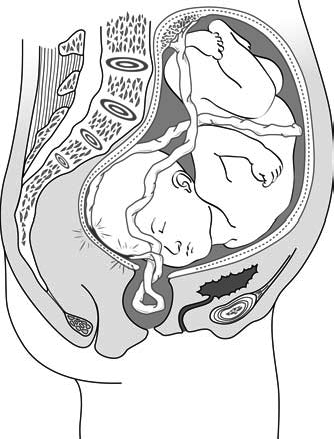
Compression of the cord between maternal tissues and the foetus (Figures 5.11 and 5.12) during contractions causes foetal distress and rapid foetal death.
Figure 5.11 - Cord coming out of the vaginal opening
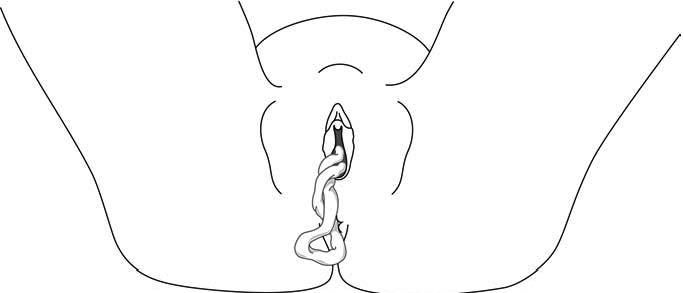
Figure 5.12 - Compression of the cord by the presenting part
5.4.1 Diagnosis
- Amniotic sac has ruptured: cord can be felt between the fingers and, if the foetus is still alive, pulsations can be felt.
- Foetal distress: foetal heart rate is slow and irregular.
5.4.2 Management
Foetus dead or nonviable (extreme premature)
No specific intervention, vaginal delivery, no caesarean section.
Foetus alive
This is an obstetric emergency, deliver immediately:
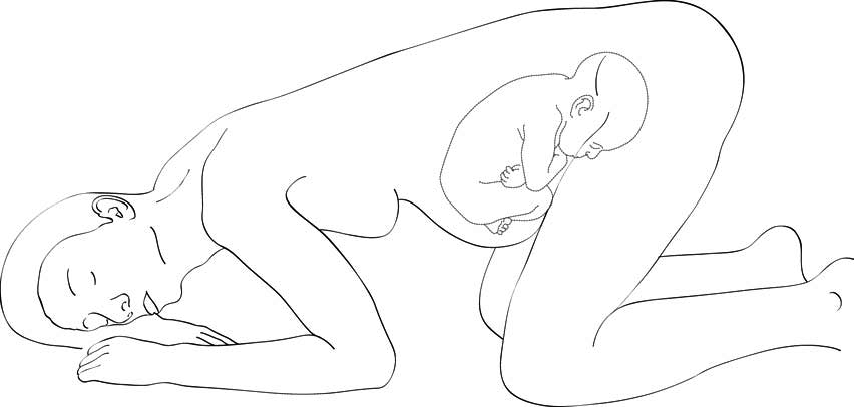
- The woman in knee-chest (Figure 5.13) or Trendelenburg (dorsal decubitus, head down) position to take the pressure off the cord.
- Manually push the presenting part toward the uterine fundus to relieve pressure on the cord. Do not remove hand until extraction of the foetus by caesarean section. If it is difficult to maintain manual elevation of the foetus through the vagina, fill the bladder with 500 ml of 0.9% sterile sodium chloride to maintain upward displacement.
- Caesarean section, holding the presenting part of the cord via the vagina until extraction. Check for foetal heart tones right before the procedure. If foetal heart tone is no longer heard, it is better to let vaginal delivery proceed (the foetus is already dead).
- If the presenting part is engaged and the cervix fully dilated, it will not be possible to push the presenting part back; perform vaginal extraction quickly: instrumental delivery (Section 5.6) or total breech extraction (Chapter 6, Section 6.3).
Figure 5.13 - Knee-chest position