The importance of logistics during a campaign is often underestimated. Good coordination between the medical and logistics teams in planning, organizing, implementing and monitoring activities is essential for:
- locating, organizing and managing the central storehouse;
- the cold chain;
- identifying and setting up the vaccination sites;
- supply;
- transport;
- communications;
- waste collection and disposal.
6.5.1 Central storehouse
Location
The best option is to have the cold chain, medical stock, logistics stock, vehicles and fuel all in the same place. All of the teams are supplied from this central point.
If it is impossible to find a large enough space, make sure to find spaces that are near each to other to facilitate organisation and supervision.
If possible, choose a large city and a location that is accessible at all times, with round-theclock electricity to ensure continuous cold production (refrigeration and freezing).
Layout
The central storehouse is laid out in five sectors of varying floor space:
- Active cold chain (freezers, refrigerators and cold room): 0.3 m3/1,000 doses
- Passive cold chain: 2.85 m2/vaccination team
- Renewable medical equipment and supplies: floor space depends on estimated needs
- Logistics equipment and supplies: floor space is a function of estimated needs
- Vaccination module preparation area (2.5 m2/team)
Management
Stock management is entrusted to a trained manager, aided by one or more assistants. Each person’s tasks are clearly defined. One of the assistants should be able to fill in for the manager in case of absence.
The practical details of stock management and the schedule of activities (ordering, distributing and monitoring stock) should be established in advance in a way that distributes the workload appropriately.
Management tools
Stock card
The stock card (Appendix 32) is essential for inventory monitoring and product traceability. Each item (vaccines, diluents, drugs, supplies and kits) has its own stock card, which is updated every time items go in or out.
The card must include:
- The International Non-proprietary Name (INN) of the product, the form, dosage, lot number and expiry date. Quantities of vaccines are always expressed in number of doses, not in number of vials.
- Stock movements (stock in and origin, stock out and destination) and dates. Enter each movement on its own line, even if there are several movements in the same day.
- Orders placed and dates. When an order is placed, the date, name of the supplier and quantity ordered are entered but the “STOCK” column remains unchanged. When the order arrives, the quantity received is entered in the “IN” column and the “STOCK” column is updated.
- Inventories and dates. If the cards are kept correctly, the “STOCK” column corresponds to the inventory. Any differences should be investigated.
The card may also include other information, such as:
- buffer stock/maximum stock;
- other storage locations for the product;
- unit price.
To prevent inventory shortages, an alert threshold is defined for each “sensitive” item and noted on the stock card. It is calculated based on the consumption, the supply time and a reserve.
For example, if it takes a product one month to arrive after being ordered, the alert threshold is equal to one month’s consumption + a one-month reserve = 2 months.
Monitoring table
In addition to stock cards, a monitoring table for sensitive items (vaccines, auto-disable syringes, dilution needles and syringes and safety boxes) should be displayed and updated daily.
Delivery forms
Delivery forms (Appendix 33) are pre-printed to make the work easier and prevent transcription errors. Signed copies of these documents are kept by the storekeeper and person in charge at each site.
6.5.2 Cold chain
Centrally
There should be a generator in case of power outages (or a backup generator if the electrical power source is a generator).
A technician (aided, if necessary, by an assistant) is responsible for:
- installing refrigerators and freezers and turning them on at least 24 to 48 hours before vaccines arrive;
- appliance operation, maintenance and repair;
- monitoring temperatures;
- preparing the cold boxes and vaccine carriers for transport to the sites (cleaning and loading the ice packs and placing the thermometer in the cold boxes);
- freezing the ice packs.
Note: ice packs should be frozen several days before the campaign starts, and there should be enough stock for the entire campaign. To freeze ice packs more quickly, freeze half of them in the morning and the other half at night.
A pharmacist (or member of the medical staff) is responsible for:
- managing the stock of vaccines and diluents;
- preparing the vaccines and diluents that are sent to the vaccination sites daily;
- checking the unused vaccines and diluents at the sites, which are put back into stock.
Notes:
- All of the vaccines sent to a vaccination site should be from the same lot, and the same for diluents. Do not mix products from different lots.
- During the campaign, diluents should be chilled (in a refrigerator or cold box) for at least 12 hours before use.
Vaccination sites
At the sites, vaccines are stored in a cold box and/or vaccine carrier.
The ice packs should be replaced:
- once a day for vaccine carriers;
- every other day (or more often, depending on the outside temperature) for cold boxes.
Note: the time needed to re-freeze ice packs can be reduced by storing the partially-thawed ice packs in an insulated container.
For vaccine storage at the site, see Appendix 34.
6.5.3 Vaccination sites
Distribution and number
The number of sites is calculated based on the size of the target population.
Their distribution depends on the population density, the size of the area and the accessibility, but they should cover all neighbourhoods/villages. In densely population areas, one site can cover up to 15,000 residents.
Note: the greater the number of sites, the more challenging the logistics (transport, supply, cold chain, etc.). While some sites can accommodate two teams, with more than two teams the crowd becomes to hard to control. It is better to open another site.
Selection criteria
Depending on the context (rural area, urban area, refugee camp), a vaccination site can be a community hall, school, place of worship, tent or shaded outdoor area. Avoid health care facilities so as not to disrupt normal activities.
- The site must be easily accessible (main roads).
- The area should be large enough to allow a smooth flow of people to be vaccinated and a comfortable, practical layout for the teams. Too large a site is hard to organise (confusion on where to go, security, etc.).
- The waiting area should be shaded and large enough for a roughly 50-metre queue.
- Using a building with a separate entrance and exit is essential in preventing jostling.
- Use an enclosed site (walls or fences), if possible, because it is easier to channel the population when there is a large crowd.
Organizing the site
Prepare the site and all the necessary equipment the day before the campaign starts. Security and a smooth flow of traffic are essential, especially during the first 2 days when the crowds are largest. Do not start the vaccination until everything is ready.
Set-up
- Outdoor sites should be used in rural areas only.
- If the site is not enclosed, mark it off using a rope or safety fencing.
- Organise the queues using rope or barrier tape. Allow about a 50-metre queue, narrow enough to allow only one person at a time to pass. A line that zigzags is better than a straight line, because it reduces the press of the crowd.
- Provide drinking water in the waiting area, as some people may come from far away.
- If the site is very large, mark off the entire flow path inside with ropes, from the entrance to the exit, and position security guards to ensure a smooth flow of people.
- Vaccination cards are filled in at the entrance to the site.
- The preparers’ work area should be separated somewhat from the flow of people, next to the vaccinator.
- The tally sheets are completed right after the vaccination.
- Equipment and supplies should be out of the population’s reach, but easily accessible to the preparers.
- The waste storage area should be some distance away and protected.
Figure 6.1: Layout of a 2-team vaccination site
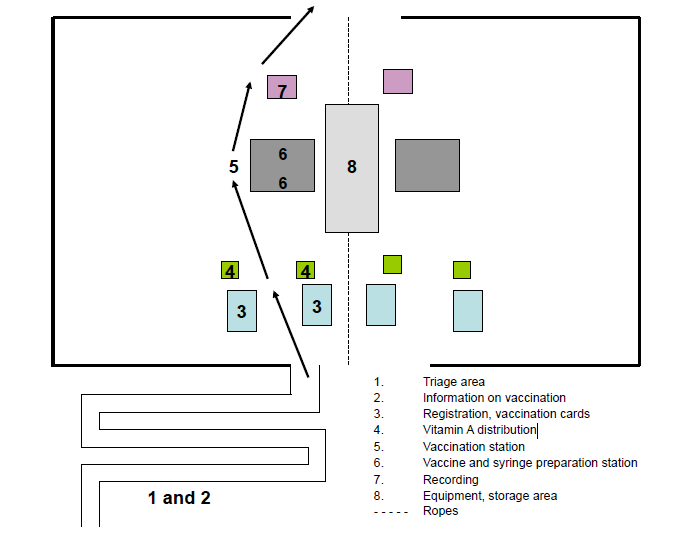
Also see Appendix 36 for a summary of how a vaccination site is organized.
6.5.4 Supply
A module-based supply system facilitates preparation and distribution. The modules are prepared ahead of time at the central storehouse. Provide 2 types of modules:
- Equipment for one vaccination team (Appendix 37);
- Equipment for one supervision team (Appendix 38).
The modules contain:
- Renewable medical supplies and vaccines for one day. This module is prepared in advance at the central storehouse and given to each team each day. The unused stock is inspected every evening. If it is equal to or greater than the contents of one module, there is no need to resupply.
- Equipment (medical and non-medical) that is given to each team the first day of the campaign and returned at the end of the campaign. Check that the box is labelled with the team number to which it belongs.
The supplies given to each team are recorded each day, making it possible to count up all the supplies that were used at the end of the campaign, and to calculate the indicators for the evaluation (Appendix 39).
6.5.5 Organising transport
Appropriate (in number and type) and reliable transport is essential to a smoothly-running campaign.
Estimating transport needs
- Vehicle needs are estimated based on:
- the number and location of sites;
- the number of teams and the duration of the campaign;
- the number of supervision teams and their schedule;
- the condition of the roads (urban and rural areas);
- how supply is organized.
Have one lorry for delivering supplies.
Have cars, motorcycles, bicycles or other means of transport for deploying vaccination and supervision teams.
If possible, have one vehicle exclusively for waste collection.
- Fuel needs are estimated based on:
- the average consumption per vehicle;
- the estimated mileage (anticipated schedule);
- the condition of the roads.
Inventory of available resources
- Cars and lorries:
- type (break, minibus, etc.) and model (city or all-terrain);
- operating condition and reliability;
- type of fuel and fuel consumption;
- number of seats and possibility of transporting supplies;
- assignment of a driver or not;
- lending agency or organization, duration and conditions of loan;
- rental conditions (cost, insurance, etc.).
- Fuel: type and availability (quantity, location), quality and cost.
Team transportation
Transportation must be appropriate to the teams’ activities (vaccination, supervision, logistics or mobilisation) and the field conditions (distances, road conditions, etc.). Means of transport may be obtained from the health or administrative authorities and partners, or rented for the duration of the campaign.
In urban areas, the vaccination teams get to the sites on their own, or group transport is arranged.
The opening times for the different sites can be staggered to optimise and rationalise transportation for the teams.
In rural areas the sites are often remote and teams must be self-sufficient. Each team needs its own vehicle.
The supervision and logistics teams must be completely self-sufficient and have their own vehicle.
Transport and delivery of equipment and supplies
There are several possibilities:
- Before or at the start of the campaign
All vaccination supplies can be stored on-site before the site opens, or each team can bring its supplies when it opens the site.
When setting up the site, it is generally possible (and preferable) to procure certain items (tables and chairs) on-site.
- During the campaign
The teams bring their supplies with them each day, or the supplies are delivered to the teams each day (or every two or three days) from the central storehouse or some intermediate, outlying storehouse when distances are large.
Whatever the options chosen, supplies must be available at the sites at all times.
Automobile fleet monitoring tools
These tools must be put in place before the campaign starts. They facilitate fleet management: vehicle monitoring/allocation table; fuel consumption monitoring table (Appendix 40).
6.5.6 Communications
The use of mobile phones, radios or other means of communication facilitates organisation and reduces travel.
6.5.7 Waste management
Mass vaccination campaigns generate a large amount of waste. The waste circuit must be well-organized and safe at every level. Waste collection and disposal should be supervised, and be evaluated when the campaign is over.
Before the campaign starts:
- Inquire about the national policy on waste treatment and disposal.
- Estimate the expected volume of each type of waste.
- Evaluate the technical resources needed (reduction, incineration, burial, encapsulation; personal protective equipment, etc.) based on the estimated volumes.
- Determine the resources available in the area in question (equipment, existing orpotential sites).
- Decide on the general organisation of treatment/disposal: centralised and/or on-site, temporary storage, transport, etc.
- Determine the number of people needed, their duties, and the training needs (safe handling of waste, AEB procedures, etc.).
Organisation of waste treatment/disposal
Centralised system
All waste is transported to a central site, where it is disposed of.
Centralising all waste at one site that has effective treatment/disposal resources is the best option.
To store waste at a vaccination site prior to transport to the disposal site, provide a secure covered area not accessible to the population.
During transport to the disposal area, staff should use the same protective equipment as for all other handling.
As far as possible, one vehicle should be allocated specifically to transporting waste. If the situation does not allow this (number of sites, number of teams or duration), make sure that personnel do not come in contact with waste during travel.
Safety boxes should be transported in a way that prevents any risk of needle stick injury or spill (properly closed, boxes taped shut, padlocked metal trunk, etc.).
To store waste at the disposal site, provide a secure area (covered, enclosed and locked).
On-site disposal
It may be that not all waste can be transported to the central disposal site. In that case, safe disposal of some waste is possible at a temporary site inaccessible to the population.
Soft waste can be disposed of right at each vaccination site.
Safety boxes should preferably be disposed of at a central location. If transporting them is too complex and/or dangerous, however, they can be destroyed on-site.
Note: empty or partially used vaccine and diluent vials are always collected, centralised and destroyed at a single controlled destruction site. They should never be destroyed on-site.
Table 6.3: Advantages and disadvantages of waste disposal strategies
| Advantages | Disadvantages | |
|---|---|---|
|
Central |
|
|
|
On-site |
|
|
For disposal techniques, see Public Health Engineering in precarious situations, MSF.
In all cases, teams should leave never the vaccination site until all waste has been taken away or destroyed.
Sorting waste
Waste is sorted by type as it is produced, and gathered in a single location.
Table 6.4: Waste management by type
| Type of waste | Collection | Disposal | |
|---|---|---|---|
| Soft waste |
Gloves, cotton wool, needle caps, packaging, etc. |
Rubbish bin |
Burned in a volume reducer/incinerator and ashes buried If bags are used, make sure that they fit into the volume reducer/incinerator’s combustion chamber when they are full. |
| Sharps |
ADS, dilution syringes and needles |
In safety boxes |
Burned in a safety box reducer and the remnants encapsulated |
| Empty vials (vaccines and diluents) | In their original packaging or in separate containers (one for vials, one for diluents) | Crushing and/or encapsulation | |
|
Other high risk waste |
Vials containing reconstituted vaccine |
In vaccine carriers |
Encapsulation |