6.6.1 Vaccine quality
At each level (capital, peripheral areas):
- For vaccines: check the name, where the delivery originated, the product quality, the label, the expiry date, the quantity delivered and the lot number. If in doubt, contact the pharmacist.
- The composition and volume of diluent can vary. Check that the diluent supplied corresponds to the vaccine (type, labelling, quantity and expiry date) and use only diluent provided by the manufacturer. In case of accidental loss of diluent, contact the pharmacist or manufacturer for advice on what to do.
- Any reconstituted vaccine vials not used within 6 hours must be discarded.
- Reconstituted vials must be kept in the cold chain between +2 and +8°C (in the slit in the foam) and protected from light.
- The first time a vaccine is received or when receiving a vaccine from a different manufacturer, read the package insert to learn the specifics about the product.
- Examine the products (the diluent should be clear and have no sediment).
- Check to make sure there was no cold chain failure during vaccine transport and storage: the vaccine vial monitor (VVM) (Appendix 41) and other temperature monitoring tools used.
Note: Measles vaccines are not sensitive to freezing, but exposure to temperatures over +8°C can rapidly reduce vaccine effectiveness after reconstitution. If there has been a break in the cold chain, quarantine the vaccines in a refrigerator between +2°C and +8°C, marked “DO NOT USE”, until the pharmacist in charge decides whether they can be used or not. Fill out the cold chain failure report (Appendix 42).
The cold chain report:
- Describes the incident: location, date, circumstances, cause of problem, actions taken, name of person reporting.
- Details:
- The list of products with the manufacturer’s name, the lot number and the quantities
- The indications given by the temperature monitoring tools (Log Tag®, thermometer, VVM, etc.)
Quarantined vaccines may not be used until the person in charge gives authorisation after analysing the report.
6.6.2 Injection safety
Aseptic technique must be used at every step (vaccine reconstitution, syringe preparation and storage). See Appendix 34.
Ask about any injection safety problems during previous campaigns.
To ensure injection safety:
- Use only auto-disable syringes with a fixed needle to administer the vaccine. These are single-use and impossible to reuse.
- Collect, transport, and dispose of waste in an appropriate manner.
Follow the bundle policy for supply:
Orders and funding routinely include vaccines
+ auto-disable syringes + syringes for reconstitution
+ sharps collection and disposal containers (safety boxes).
- Educate all personnel on the risks of technical errors:
- Infection of personnel due to accidental needle stick
- Local infection due to nonsterile injection (handling error during preparation or injection)
- Viral transmission (hepatitis B and C and HIV) due to reuse of injection supplies
- Vaccine inefficacy due to reconstitution error or storage problem
- Monitor best practices using the supervision grid (Appendix 35).
6.6.3 Surveillance of adverse events following immunisation (AEFI)
[1]Citation 1.World Health Organization. Prequalified Vaccines. WHO - Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunisation Devices, Vector Control).
https://extranet.who.int/prequal/vaccines/prequalified-vaccines
AEFI surveillance applies to everyone vaccinated against measles during the campaign that experiences one or more symptoms, appearing within 30 days of vaccination, that might be related to it.
AEFIs are detected by passive surveillance that begins the first day of vaccination. Health care personnel are trained and definitions, tools and a reporting circuit are put in place.
Health care personnel are trained to quickly detect and appropriately manage an anaphylactic reaction at the site. Each team is equipped with an ampoule of epinephrine (adrenaline), a 1 mL syringe and an intramuscular needle to administer the epinephrine (Appendix 43) before transferring the person to the hospital.
AEFIs must be reported (Appendix 44 and Appendix 45). Serious AEFIs must be reported immediately for investigation and confirmation of the link to the vaccination.
Find out from the national immunisation programme how AEFIs are classified in the country. The WHO recommends the following classification
[2]Citation 2.World Health Organization. Global manual on surveillance of adverse events following immunization. WHO; May 2016. Accessed March 21, 2025.
https://www.who.int/vaccine_safety/initiative/en/
:
Vaccine product-related reaction: An AEFI caused or precipitated by a vaccine, due to one or more of the inherent properties of the (correctly administered) vaccine product.
Vaccine quality defect-related reaction: An AEFI caused or precipitated by a vaccine that is due to one or more quality defects of the vaccine product, including its administration device as provided by the manufacturer.
Immunisation error-related reaction: An AEFI caused by inappropriate vaccine handling, prescribing or administration and thus by its nature preventable.
Immunisation anxiety-related reaction: An AEFI arising from anxiety about the immunisation.
Coincidental event: An AEFI caused by something other than the vaccine product or immunisation error but a temporal association with immunisation exists.
6.6.4 Prevention and control of infections
There are a number of AEB-related risks:
- For vaccinators, the risk is high due to the large number of injections being administered at a sustained pace. To reduce the risks:
- Enlist the help of the person accompanying the child:
- Prepare a suitable space: chair for the person accompanying the child
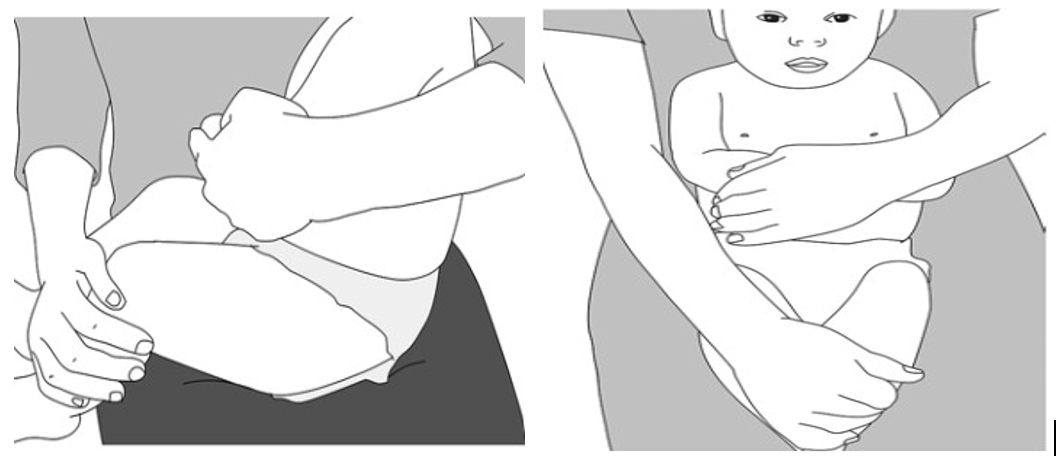
- Clearly explain the importance of holding the child and how to do it (see figure 6.2) [3]Citation 3.World Health Organization. Immunization in practice: a practical guide for health staff, 2015 update. WHO; 2015. https://www.who.int/immunization/documents/ISBN_9789241549332/en/.
- Wearing disposable gloves is not necessary, since the WHO does not consider the risk of body fluid exposure significant [4]Citation 4.World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. WHO; 15 Jan. 2009. https://www.who.int/publications/i/item/9789241597906 .
- Regular handwashing is essential (set up the means to do so at the vaccination site).
- Enlist the help of the person accompanying the child:
- For logistics teams, accidents are due to incorrect use of safety boxes (filling them beyond the line, failing to close them completely), to waste sorting errors (needles thrown into rubbish bags, for example) or to unprotected transport of waste (not separate from people). Wearing personal protective equipment is compulsory (this equipment is included in the vaccination kit):
- For waste collection: thick gloves (work gloves, at a minimum), coveralls with long sleeves and legs, and boots
- For waste disposal: thick gloves, leather apron, coveralls with long sleeves and legs, boots, and after assessing the risk and depending on the disposal method, safety glasses and a mask.
All personnel should already know what to do in case of AEB when the campaign begins.
A physician consultant is designated to:
- Evaluate the risk for people who are exposed, decide whether to treat, and provide follow-up (Appendix 46)
- Fill out and/or centralise the AEB report forms (Appendix 47)
- Ensure that AEB kits are always available
A handwashing station and a bottle of 10% polyvidone iodine should be available at each vaccination site and waste storage/disposal area for topical treatment (Appendix 46).
Figure 6.2 – How to hold a child during vaccination [3]Citation 3.World Health Organization. Immunization in practice: a practical guide for health staff, 2015 update. WHO; 2015. https://www.who.int/immunization/documents/ISBN_9789241549332/en/.
- 1.
World Health Organization. Prequalified Vaccines. WHO - Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunisation Devices, Vector Control).
https://extranet.who.int/prequal/vaccines/prequalified-vaccines - 2.
World Health Organization. Global manual on surveillance of adverse events following immunization. WHO; May 2016. Accessed March 21, 2025.
https://www.who.int/vaccine_safety/initiative/en/ - 3.
World Health Organization. Immunization in practice: a practical guide for health staff, 2015 update. WHO; 2015. https://www.who.int/immunization/documents/ISBN_9789241549332/en/.
- 4.
World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. WHO; 15 Jan. 2009. https://www.who.int/publications/i/item/9789241597906