Example 1 – Major African city, 2010
(source: MSF)
The city had an estimated population of 1,133,794.
The last measles outbreak occurred in 2005, with 8,015 reported cases (attack rate = 660/100,000). A vaccination campaign targeting children ages 6 months to 5 years was conducted in 2006.
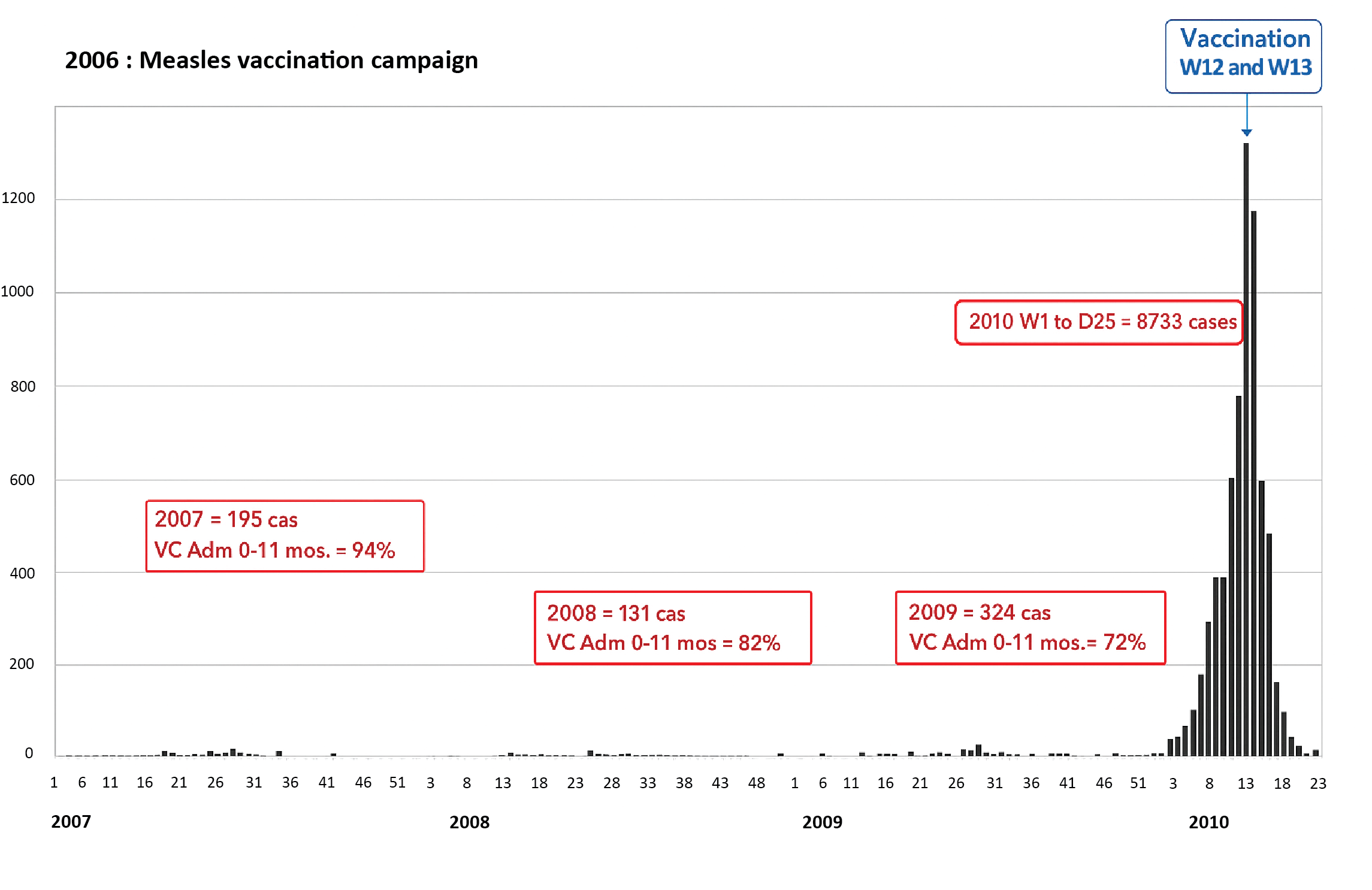
The curve shows that:
- From 2007 to 2009, there were few reported cases and the routine vaccination coverage (VC) dropped year by year.
- In 2008, a vaccination campaign (SIA) was conducted in all districts. The overall VC was an estimated 68% (90%, 71%, 68% and 63% in the northern, southern, central and eastern districts, respectively).
- In early 2010 there was an increase in the number of cases: 689 cases from Week 1 to 7, with an attack rate that was four times higher than in previous years. There were significant disparities between districts; the attack rate in the eastern district was 6.3 times higher than in the northern district, 1.8 times higher than in the southern district, and 1.5 times higher than in the central district.
- In Week 7, an investigation was conducted and the expanded programme of immunisation (EPI) reinforced.
- Despite this intervention, the number of cases increased, reaching a peak in Week 12.
A total of 8,733 cases and 32 deaths were reported from Week 1 to Week 25. The outbreak lasted sixteen weeks.
Number of measles cases per week, 2007 to 2010
Several actions were taken in response to this outbreak:
- Beginning at Week 7: reinforcement of EPI for children ages 9-11 months
- From Week 12 (10 weeks after the start of the outbreak) to Week 15, non-targeted mass vaccination campaign for children ages 6 months to 15 years
A vaccination coverage survey assessed the VCs before and after the mass vaccination campaign:
Before the campaign, overall VC for children ages 6 months to 15 years: 70.4%
(95% CI: 68.5%-72.3%)
After the campaign, overall VC for children ages 6 months to 15 years: 82.5%
(95% CI: 81.5%-83.5%)
The main reasons for non-vaccination were: practical reasons (37%), vaccination refusal (25%), lack of information (14%), previous vaccination (1%), and no explanation (16%).
Key points
The VC (EPI + mass vaccination campaign) was inadequate and allowed a recrudescence of cases in early 2010 (even larger in neighbourhoods where vaccination coverage was lowest).
Reinforcing EPI activities did not prevent an epidemic.
The belated outbreak response vaccination (10 weeks after the epidemic started) helped control its spread (incidence fell in the weeks that followed), and the outbreak ended around Week 22.
Example 2 – A rural health zone, Central Africa, 2022
(source: MSF)
The zone had an estimated population of 308,873. It is a rural zone (population density 38 per km2) with 19 administrative subunits.
The last measles outbreak was in 2019; the Ministry of Health organised a response for children ages 6 to 59 months.
The administrative routine EPI vaccination coverage for the measles vaccine (MCV) was 98.8%, but the EPI suffered a 75-day MCV shortage in 2021.
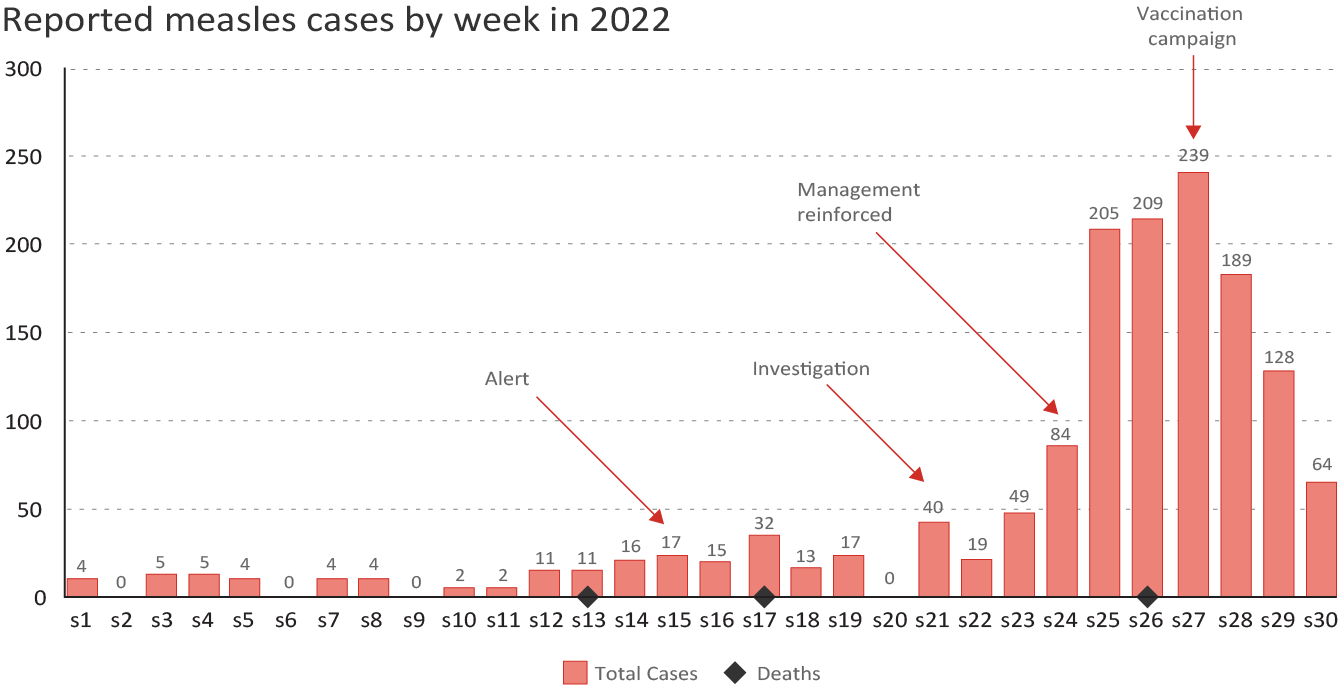
Starting in Week 1, sporadic cases were being reported in the zone, many in places that were difficult for the MoH surveillance team to access.
By Week 15, the alert threshold (defined in this context as 35 cases in 3 weeks) had been passed and the case fatality rate was high (12.5%); laboratory confirmation was not available.
In Weeks 20/21, the MoH and MSF conducted a joint investigation showing significant underreporting of cases and confirming the measles outbreak (increasing number of cases in 12 administrative subunits visited), with 79% of the cases under age 5 years and 80% of the samples positive for measles in Week 18.
Actions taken in response to this outbreak:
- Health promotion and community engagement: information, active measles case-finding, and community mobilisation two weeks before the vaccination campaign
- Management activities were then reinforced: active case-finding, treatment kits donated to the peripheral clinics, and a measles treatment centre set up (Week 24)
- A non-targeted measles vaccination campaign for children ages 6 to 59 months (Week 27) with 111% vaccination coverage
- Other jointly conducted activities: vitamin A distribution, MUAC measurement for children under age 5 years and vaccination for other immunisation schedule diseases for children under age 2 years
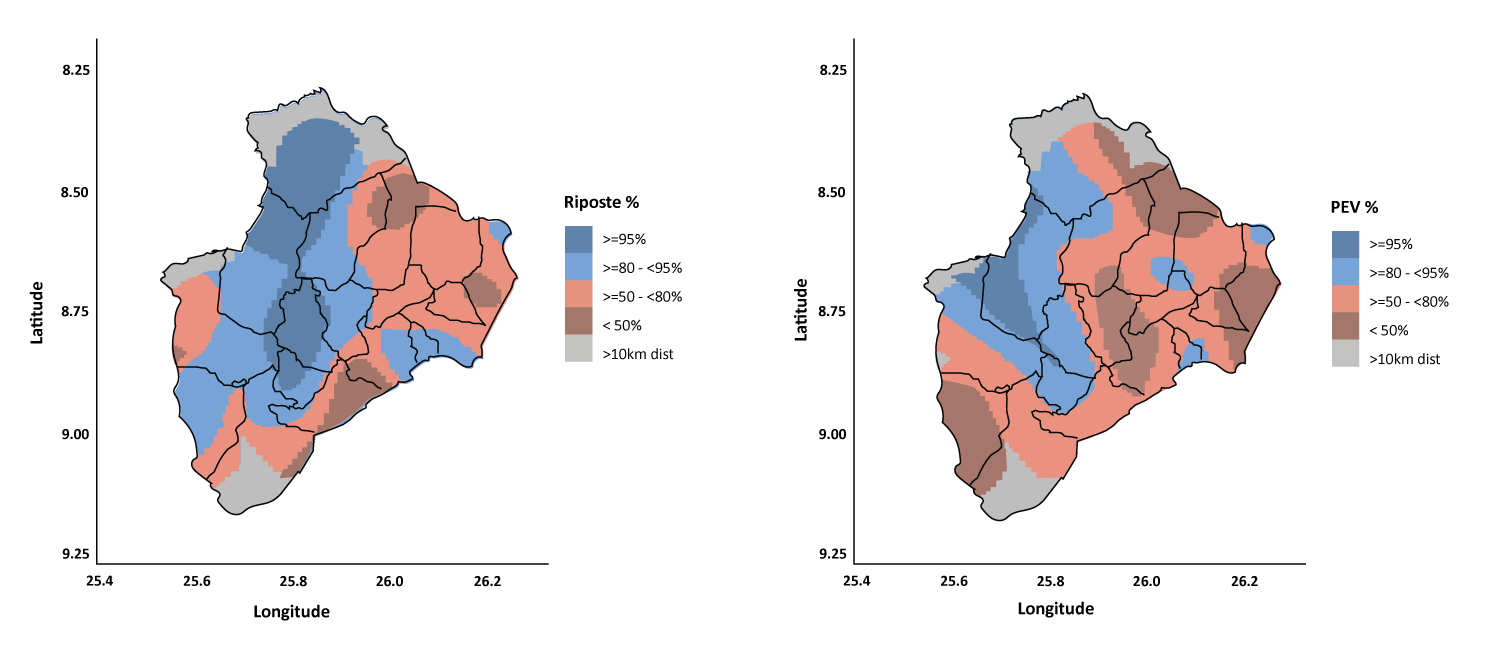
A vaccination coverage survey showed the following VCs:
MSF/Epicentre.
- Measles outbreak response campaign: VC 80.5% (86% in easily accessible areas and 71% in difficult-to-access areas). The main reasons for non-vaccination for the outbreak response campaign were as follows: absent at the time of the campaign, 27%; vaccination refusal, 25%; lack of information, 14%.
- EPI vaccination: VC 70% in easily accessible areas and 60% in difficult-to-access areas.
A drop in the number of cases was noted two weeks after the outbreak response campaign (conducted 12 weeks after the alert). There was no recrudescence of cases in the weeks that followed.
Key points
Three years after the previous outbreak, despite reportedly good administrative VCs, there was a recrudescence of cases.
Once the first cases were investigated and management support was set up, it became clear that cases were being significantly under-reported.
The response campaign helped bring the outbreak under control quickly.
The vaccination coverage survey highlighted the non-uniformity of the vaccination campaign, giving a better understanding of the outbreak’s causes to help tailor future vaccination strategies.