Download 'Patient management' (PDF document)
13.1 Management
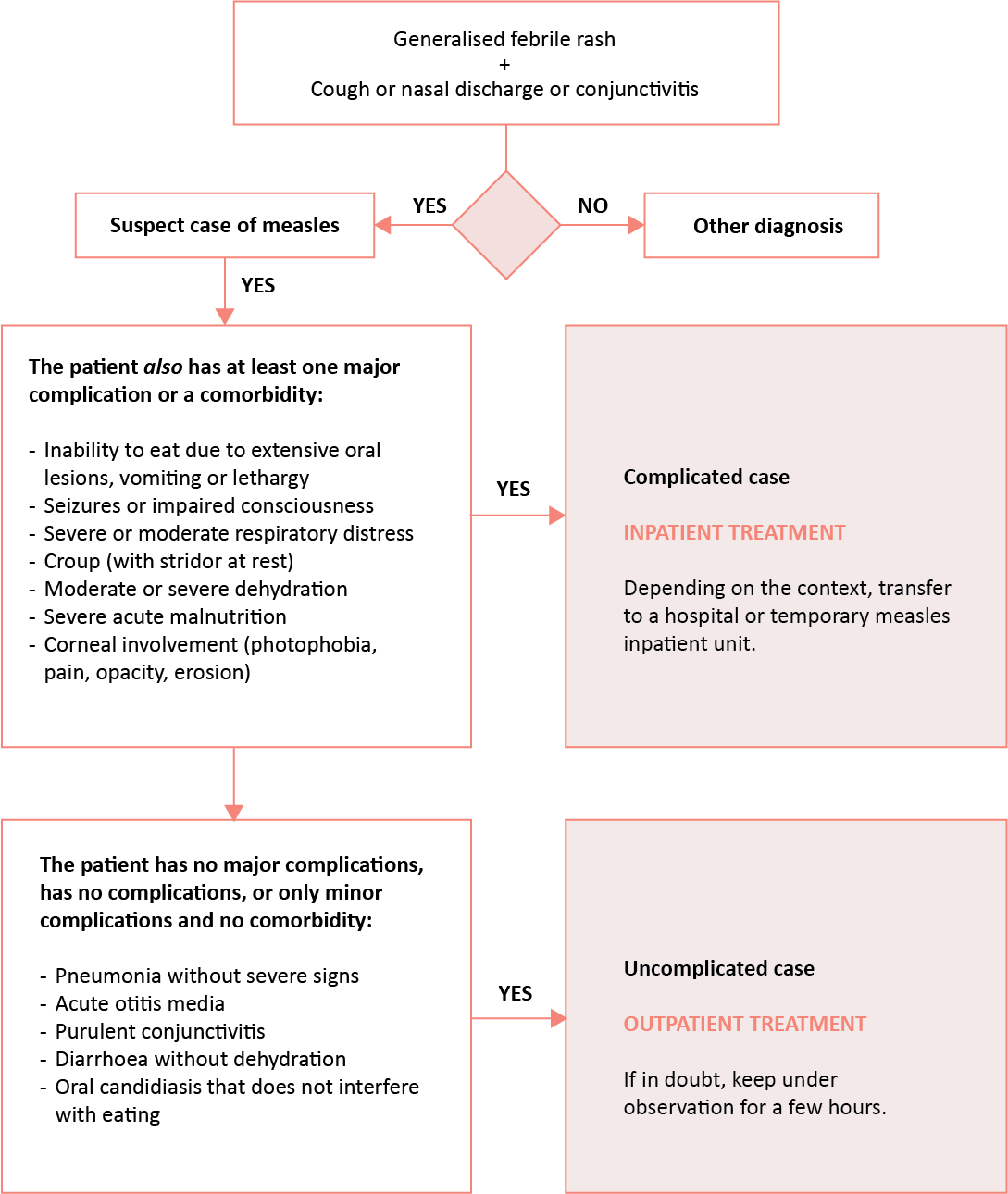
13.2 Case management
13.2.1 Uncomplicated cases (outpatient treatment)
Standard treatment
- Paracetamol PO :
Child < 1 month: 10 mg/kg 3 or 4 times daily (max. 40 mg/kg daily)
Child ≥ 1 month: 15 mg/kg 3 or 4 times daily (max. 60 mg/kg daily)
Adult: 1g 3 or 4 times daily (max. 4 g daily)
| Age | < 1 mo. | 1 to < 3 mo. | 3 mo. to < 1 yr | 1 to < 3 yr | 3 to < 5 yr | 5 to < 9 yr | 9 to < 14 yr | ≥ 14 yr Adult |
|---|---|---|---|---|---|---|---|---|
| Weight | < 4 kg | 4 to < 6 kg | 6 to < 10 kg | 10 to < 15 kg | 15 to < 20 kg | 20 to < 30 kg | 30 to < 50 kg | ≥ 50 kg |
| 120 mg/5 mL susp. | 1.5 mL x 3 | 2.5 mL x 3 | 4 mL x 3 | 6 mL x 3 | 8 mL x 3 | 12 mL x 3 | - | - |
| 100 mg tablet | - | ½ tab x 3 | 1 tab x 3 | 1½ tab x 3 | 2 tab x 3 | 3 tab x 3 | - | - |
| 500 mg tablet | - | - | - | - | - | - | 1 to 1½ tab x 3 | 2 tab x 3 |
- Amoxicillin PO : for 5 days
Child: 30 mg/kg (max. 1 g) 3 times daily
Adult: 1 g 3 times daily
| Age | < 3 months | 3 to 23 months | 2 to 7 years | ≥ 8 years and adult |
|---|---|---|---|---|
| Weight | < 6 kg | 6 to 11 kg | 12 to 24 kg | ≥ 25 kg |
| Daily dose | 125 mg x 3 | 250 mg x 3 | 500 mg x 3 | 1 g x 3 |
| 125 mg/5 mL susp. | 5 mL x 3 | 10 mL x 3 | 20 mL x 3 | - |
| 250 mg tablet | ½ tab x 3 | 1 tab x 3 | 2 tabs x 3 | 4 tabs x 3 |
| 500 mg tablet | - | - | 1 tab x 3 | 2 tabs x 3 |
- Retinol* (vitamin A) PO : one dose on D1 and D2 aCitation a.In pregnant women (ask the patient), give lower dose: 25 000 IU once weekly for 4 weeks.
| Age | < 6 months | 6 to 11 months | 1 year and more |
|---|---|---|---|
| Weight | < 7.5 kg | 7.5 to 9 kg | 10 kg and more |
| Dose | 50 000 UI | 100 000 UI | 200 000 UI |
| 200 000 IU capsule (8 drops) | 2 drops | 4 drops | 1 capsule |
* Except in pregnant women
- Wipe eyes with cotton and clean water
- Keep nasal passages clear (using a tissue or by nasal lavage with 0.9% sodium chloride if appropriate)
- Depending on the context, for children < 5 years, food supplement: 500 kcal daily, ready-to-use food, for 2 weeks
Treatment of minor complications
- Pneumonia without severe signs: amoxicillin PO, 30 mg/kg (max. 1 g), 3 times daily, 5 days
- Acute otitis media: child > 5 years; treat fever and pain, reassess after 48 hours to decide if antibiotic treatment is needed (amoxicillin PO 5 days)
- Mild croup: dexamethasone PO (2 mg tablet): 0.6 mg/kg (maximum 16 mg), single dose or prednisolone PO (5 mg tablet): 1 mg/kg, single dose
- Purulent conjunctivitis: clean the eyes with clean water + 1% tetracycline eye ointment (2 times daily, 7 days)
- Bitot’s spots: retinol PO one dose (see above) on D1, D2, 3rd dose 4 to 6 weeks later
- Oral candidiasis: nystatin 100 000 IU/ml oral suspension (1 mL 4 times daily, 7 days)
- Diarrhoea without dehydration: WHO plan A (see Appendix 14)
13.2.2 Complicated cases (inpatient)
Systematic standard treatment (see above)
- Paracetamol PO : see above
Paracetamol IV 10 mg/mL, 50 mL or 100 mL bag or
Vial If oral administration is not possible (repeated vomiting or impaired consciousness together with severe hyperthermia), maximum 72 hours.
| Weight | < 10 kg | 10 to 49 kg | ≥ 50 kg |
|---|---|---|---|
| Dose to be administered every 6 hours (in mg) | 10 mg/kg | 15 mg/kg | 1 g |
| Dose to be administered every 6 hours (in mL) | 1 mL/kg | 1.5 mL/kg | 100 mL |
| Maximum dose | 30 mg/kg/daily | 60 mg/kg/daily | 4 g/daily |
Administer paracetamol IV infusions every 6 hours. Each dose in administered over 15 minutes.
Change to oral route as soon as possible.
Respiratory and ENT complications
Severe pneumonia
- Oxygen if cyanosis or SpO2 < 90%
- Amoxicillin 1 g/clavulanic acid 200 mg powder, IV infusion over at least 30 minutes
- Child aged 1 to 3 months: 30 mg/kg every 12 hours, to be administered via syringe pump or pediatric infusion set
- Child over 3 months: 30 mg/kg every 8 hours, to be administered by IV infusion
Reconstitution for IV use:
| Vial | Solvent to add | Volume to add | Final amoxicillin concentration |
|---|---|---|---|
| 1 g/200 mg | WFI | 19.1 mL | 50 mg/mL |
- Compatible solutions (diluent): 0.9% NaCl or Ringer Lactate
| Do not use glucose solution (risk of precipitation) |
- Alternative: ceftriaxone 1 g, IV or IM bCitation b.During an epidemic, ceftriaxone can be considered a first-line option because it is easier to use, allowing a single daily dose administered IM. This is why ceftriaxone is included in the example donation kit for the management of severe cases (see Appendix 10).
- Child under 50 kg: 80 mg/kg (max. 4 g), once daily
- Child 50 kg or more / adult: 1–2 g, once daily
| Age | 1 to 11 months | 1 to 4 years | 5 to 10 years | 11 to 15 years | Adult |
| Weight | 4 to 9 kg | 10 to 19 kg | 20 to 29 kg | 30 to 50 kg | > 50 kg |
| Dose | 300 to 700 mg | 800 to 1500 mg | 1.6 to 2.3 g | 2.4 to 4 g | 1 to 2 g |
IV injection: dissolve powder (1 g) in 10 mL of water for injection, withdraw the volume corresponding to the dose, then:
- If dose < 500 mg, dilute in 15 mL of solution (0.9% NaCl or 5% or 10% glucose)
- If dose 500 mg to 1 g, dilute in 25 mL of solution (0.9% NaCl or 5% or 10% glucose)
Administer preferably with a syringe pump or pediatric infusion set over 30 minutes, or if not possible, as a slow IV injection over 5 to 15 minutes with caution (risk of seizure if injected too fast).
Injection IM
- Ceftriaxone 1 g powder + 3.6 mL water for injection to obtain a concentration of 250 mg/mL.
Administer the reconstituted volume adapted to the child’s weight without further dilution. - Or ceftriaxone 1 g powder vial + lidocaine for IM injection.
| Vials for IM injection are provided with a specific lidocaine solvent. Once reconstituted with this solvent, ceftriaxone must only be used IM, NEVER IV. |
Add the lidocaine solvent supplied by the manufacturer to the 1 g vial.
Always check the presentation, as dosage and solvent volume vary by manufacturer.
If the injection volume is large, divide the dose between both buttocks.
If no improvement after 48 to 72 h, reassess potential complications such as empyema and treat accordingly:
If treatment started with ceftriaxone 80 mg/kg once daily:
- Add clindamycin IV, 10 mg/kg every 8 hours
- If treatment started with amoxicillin/clavulanic acid, switch to ceftriaxone IV or IM (as above) + clindamycin IV, 10 mg/kg every 8 hours
- Clindamycin IV, 2 mL vial, equivalent to 150 mg base/mL:
- Dilution
- If dose < 250 mg, dilute in 15 mL of compatible solution (0.9% NaCl, 5% or 10% glucose, or Ringer Lactate)
- If 250 mg ≥ dose < 500 mg, dilute in 30 mL of compatible solution
- If dose ≥ 500 mg, dilute in 50 mL of compatible solution
- Infusion: via syringe pump/pediatric infusion set over 30 to 60 minutes
- Dilution
If the patient’s clinical condition improves and oral intake is possible, switch to oral antibiotics to complete an effective 5 to 7 day course in total.
In the case of empyema, continue parenteral antibiotics for at least 7 days and until the patient has been afebrile for 3 days, then switch to oral antibiotics (if possible) to complete a total treatment of at least 14 days.
- Switching to oral therapy:
- If amoxicillin/clavulanic acid IV: amoxicillin/clavulanic acid PO (see below)
- If ceftriaxone IV or IM: amoxicillin/clavulanic acid PO
- If ceftriaxone IV or IM + clindamycin IV:
- If there is no concern for MRSA cCitation c.MRSA: Methicillin-Resistant Staphylococcus aureus. : risk: amoxicillin/clavulanic acid PO
If MRSA risk is present: cefixime PO, 10 mg/kg (max. 200 mg) 2 times daily
+ clindamycin PO, 10 mg/kg (max. 600 mg) 3 times daily
- Amoxicillin/clavulanic acid PO
- Child < 40 kg: 50 mg/kg 2 times daily
- Child or adult ≥ 40 kg:
Ratio 7:1: 2625 mg daily (1 tablet of 875/125 mg 3 times daily)
Ratio 8:1: 3000 mg daily (2 tablets of 500/62.5 mg 3 times daily)
Amoxicillin/clavulanic acid Ratio 7:1
| Age | < 2 months | 2 to 11 months | 1 to 4 years | 5 to 10 years | 11 to 15 years | Adult |
| Weight | < 5 kg | 5 to 9 kg | 10 to 19kg | 20 to 2 9 kg | 30 to 39 kg | ≥ 40 kg |
| 400:57 mg/ 5 mL oral susp. | 1 to 3 mL x 2 | 3 to 5 mL x 2 | 6 to 11 mL x 2 | - | - | - |
| 200:28.5 mg Disp. tab. | 1 tab x 2 | 1½ to 2 tab x 2 | 2½ to 4 tabs x 2 | - | - | - |
| 875:125 mg tablet | - | - | ½ to 1 tabs x 2 | 1½ x 2 | 2 tabs x 2 | 1 tabs x 3 |
Amoxicillin/clavulanic acid Ratio 8:1
| Age | < 2 months | 2 to 11 months | 1 to 4 years | 5 to 10 years | 11 to 15 years | Adult |
| Weight | < 5 kg | 5 to 9 kg | 10 to 19kg | 20 to 29 kg | 30 to 39 kg | ≥ 40 kg |
| 500:62.5 mg/5 mL oral susp. | 1 to 2.5 mL x 2 | 2.5 to 4.5 mL x 2 | 5 to 10 mL x 2 | 10 to 15 mL x 2 | - | - |
| 500/62.5 mg tablet | - | - | 1 to 2 tabs x 2 | 2 to 3 tabs x 2 | 3 tabs x 2 | 2 tabs x 3 |
Acute otitis media
- Amoxicillin PO: 30 mg/kg 3 times daily for 5 days (see above)
- If there is discharge from the ear, keep the ear clean by wiping the external auditory canal with dry cotton wool.
Croup (acute laryngotracheobronchitis)
Mild croup
- Dexamethasone PO (2 mg tablet): 0.6 mg/kg (max. 16 mg), single dose
- Or prednisolone PO (5 mg tablet): 1 mg/kg, single dose
Severe croup
- Dexamethasone PO (2 mg tablet) or IM (4 mg in 1 mL ampoule, 4 mg/mL): 0.6 mg/kg single dose (max. 16 mg)
| Weight | < 5 kg | 5 to 9 kg | 10 to 13 kg | 14 to 17 kg | 18 to 21 kg | 22 to 26 kg | ≥ 27 kg |
| Dose in mg | 2 | 4 | 8 | 10 | 12 | 14 | 16 |
| 2 mg tab PO | 1 tab | 2 tabs | 4 tabs | 5 tabs | 6 tabs | 7 tabs | 8 tabs |
| Volume for IM injection | 0.5 mL | 1 mL | 2 mL | 2.5 mL | 3 mL | 3.5 mL | 4 mL |
- Or prednisolone PO, (5 mg tablet):1 mg/kg, single dose
Epinephrine dCitation d.Although not licensed for use via nebulisation, epinephrine should be used via nebulizer in the management of severe croup. (1 mg in 1 mL ampoule, 1 mg/mL) via nebulisation: 0.5 mL/kg per dose
(max. 5 mg)
| Age | 1 month | 2 months | 3 months | 4 to 6 months | 7 to 9 months | 10 to 11 months | 1 to 4 years (a)Citation a.In children > 4 years or > 17 kg, do not exceed 5 mL. |
|---|---|---|---|---|---|---|---|
| Weight | 4 kg | 5 kg | 6 kg | 7 kg | 8 kg | 9 kg | 10 to 17 kg |
| Dosage in mg | 2 mg | 2.5 mg | 3 mg | 3.5 mg | 4 mg | 4.5 mg | 5 mg |
| Epinephrine (1 mg/mL ampoule) | 2 mL | 2.5 mL | 3 mL | 3.5 mL | 4 mL | 4.5 mL | 5 mL |
| NaCl 0.9% to add | 2 mL | 2 mL | 1 mL | 1 mL | 1 mL | - | - |
- Oxygen if cyanose or SpO2 < 90%
Ocular complications
- Corneal lesions (opacification, ulcer)
- Retinol (vitamin A) PO: one dose on Day 1, Day 2, and a 3rd dose 4 to 6 weeks later (see above for dose by age).
- In case of ocular pain:
- Child over 12 years and adult: tramadol PO 50 mg capsule: 50 to 100 mg every 6 hours (max. 400 mg daily)
- Child 6 months to 11 years: morphine immediate-release (MIR) PO, 10 mg tablet or 10 mg/5 mL oral solution: 0.15 mg/kg every 4 hours, protocol is adjusted until pain relief is obtained
- Keep the eye clean: clean with 0.9% sterile sodium chloride and apply 1% tetracycline eye ointment, 2 times daily, to prevent or treat bacterial superinfection
- Protective dressing as long as there is photophobia
- Bitot’s spots
- Retinol (vitamin A) PO: one dose on Day 1, Day 2, 3rd dose 4 to 6 weeks later, as above
Purulent conjunctivitis
- Clean the eyes with clean water 2 times daily
- 1% tetracycline eye ointment: one application 2 times daily for 7 days
Gastrointestinal complications
- Oral candidiasis
- Nystatin PO, 100 000 IU/mL oral suspension: 1 mL of oral suspension (100 000 IU) 4 times daily for 7 days. Si pas d’amélioration après 3 jours de traitement, augmenter la posologie à 200 000 UI 4 fois par jour eCitation e.If not available, gentian violet 0.25%, applied twice daily for a maximum of 5 days.
- Diarrhoea without dehydration
- WHO treatment plan A (see Appendix 14)
- Diarrhoea with dehydration
Moderate (some) dehydration: WHO treatment plan B
Severe dehydration: WHO treatment plan C
+
Zinc sultate (20 mg dispersible tablet):
Child under 6 months: 10 mg (½ tab daily) once daily for 10 days
Child from 6 months to 5 years: 20 mg (1 tab daily) daily for 10 days
In infants: place ½ or 1 tablet in a teaspoon and add a bit of water to dissolve it.
In children over 2 years: tablets may be chewed or dissolved.
Ask the parents/carers not to remove the tablets from the blister-pack ahead of time. Once a tablet is removed from the blister-pack, it must be given immediately. Zinc supplementation is unnecessary if the child is receiving nutritional treatment (F-100, Plumpy'Nut®, BP-100®).
Other complications
- Acute malnutrition
Follow the protocol for managing malnutrition (RUTF) - Seizures
Generalised seizure lasting > 5 minutes:- Diazepam, 10 mg ampoule (5 mg/mL, 2 mL): Child: 0.5 mg/kg (0.1 mL/kg) rectally, without exceeding a total dose of 10 mg/dose for children < 12 years
- Diazepam, 10 mg ampoule (5 mg/mL, 2 mL): Child: 0.5 mg/kg (0.1 mL/kg) rectally, without exceeding a total dose of 10 mg/dose for children < 12 years
For intrarectal administration, use a nasogastric tube and a syringe, introduce the end of the tube into the rectum, inject the diazepam and leave in place for 10 minutes holding the buttocks together.
| Age | 6 to 11 months | 1 to < 3 years | 3 to < 5 years | ≥ 5 years and adult |
| Weight | 7 to < 10 kg | 10 to < 14 kg | 14 to < 19 kg | ≥ 19 kg |
| Dose in mg | 5 mg | 6.25 mg | 7.5 mg | 10 mg |
| Volume to be administered | 1 mL | 1.25 mL | 1.5 mL | 2 mL |
- Or midazolam solution, 50 mg vial (5 mg/mL, 10 mL): buccal, 0.3 mg/kg (0.06 mL/kg) or IM, 5 mg vial (1 mg/mL, 5 mL): 0.15 mg/kg (0.15 mL/kg), maximum 10 mg per dose.
Withdraw the required dose using a 1 mL syringe, open the lips and slowly administer the dose of midazolam between the cheek and lower gum of the patient lying on their side.
If seizures do not stop 5 minutes after the first dose, repeat the same dose. If seizures persist, treat as convulsive status epilepticus (see Clinical and therapeutic guidelines)
If the patient is to be transferred to an inpatient unit
Start the treatment before transferring the patient to the inpatient unit and according to the distance, the time needed for transfer, and the complications found on examination:
Administer the first dose of oral paracetamol + amoxicillin or if severe pneumonia give the first dose of ceftriaxone IM or IV (if the child already has an intravenous line)
- Severe dehydration: place an IV line and transfer the patient when stable
- Moderate dehydration and fully conscious patient: give ORS to drink while being transferred.
- Corneal lesion: protect the eye with a dry dressing
Always send the patient with a transfer form indicating the reason for the referral and the treatments administered.
- (a)
In pregnant women (ask the patient), give lower dose: 25 000 IU once weekly for 4 weeks.
- (b)
During an epidemic, ceftriaxone can be considered a first-line option because it is easier to use, allowing a single daily dose administered IM. This is why ceftriaxone is included in the example donation kit for the management of severe cases (see Appendix 10).
- (c)
MRSA: Methicillin-Resistant Staphylococcus aureus.
- (d)
Although not licensed for use via nebulisation, epinephrine should be used via nebulizer in the management of severe croup.
- (e)
If not available, gentian violet 0.25%, applied twice daily for a maximum of 5 days.
- a
In children > 4 years or > 17 kg, do not exceed 5 mL.